All published articles of this journal are available on ScienceDirect.

The Effect of “High-ankle Sprain” Taping on Ankle Syndesmosis Congruity: A Cadaveric Study
Authors Info & Affiliations
Abstract
Background:
Different treatment options exist for dynamically unstable purely ligamentous syndesmotic injury, including surgery, walking boot, brace and taping.
Objective:
The main purpose of this study was to evaluate the effect of high-ankle sprain taping (ring taping) on syndesmotic stability in various ligament conditions when axial loading is applied.
Methods:
This controlled cadaveric laboratory study included ten cadaveric specimens installed in a custom-made device applying 750N of axial loading in order to simulate weight-bearing. Sectioning of syndesmotic ligaments, AiTFL and IOL, was done sequentially and CT scan images were taken with and without high-ankle sprain taping. A validated measurement system consisting of 3 lengths and 1 angle was used. Results were compared with Wilcoxon tests for paired samples and non-parametric data.
Results:
In every ligament condition (intact vs. cut), no statistically significant difference was observed between specimens, with or without high-ankle sprain taping and with or without axial loading. When the data from ankles with AiTFL and IOL ruptures were compared, the mean for length “b” without axial loading was 7.19 (±2.17), compared to 7.20 (±1.98) with axial loading (p-value = 0.905). With taping and the leg still in axial loading, the value was 7.17 (±2.09) (p-value = 0.721), which is not statistically significant.
Conclusion:
It is impossible to conclude regarding high-ankle sprain taping’s capacity to maintain syndesmosis congruity because no significant difference was observed, regardless of condition. The most important finding is that high-ankle sprain taping did not cause malreduction of the injured syndesmosis.
Level of Evidence:
Level V cadaveric study
1. INTRODUCTION
Although ankle injuries are particularly frequent, syndesmotic injuries occur only in 1% to 24% of ankle ligamentous injuries, predominantly in the professional athlete population [1-3]. In approximately 10% of ankle fractures, there is a concomitant syndesmotic injury [4, 5]. The syndesmosis is a very stable fibrous joint composed of four ligaments, the Anterior Inferior (AiTFL) and Posterior Inferior Tibiofibular Ligaments (PiTFL), as well as the Interosseous Ligament (IOL) and the Transverse Tibiofibular Ligament (TTFL) [6-13]. It is usually injured by an external rotation of the foot, causing ligaments to rupture [1, 3, 9, 10, 13]. Each ligament composing the syndesmotic joint provides some stability; however, the AiTFL, PiTFL and IOL are the major stabilizing structures [14]. The usual pattern of injury is a disruption of the AiTFL and anterior deltoid ligament followed by the IOL, TTFL and interosseus membrane [1, 3, 12]. The PiTFL and the remaining deltoid ligament require a greater force to be injured [1, 3]. Untreated syndesmotic injury can lead to chronic instability and painful symptoms as a result of degenerative changes [12, 14-17]. Diagnosis and treatment of syndesmotic injury remain controversial as there is a lack of sensitive physical examination maneuvers to assess syndesmosis stability [2, 9, 18, 19]. Furthermore, the parameters that were once diagnostic of syndesmotic injury on simple radiography are now being challenged because of the variability seen in normal syndesmosis anatomy and the difficulty to control rotation during the radiographic assessment [15, 20-24]. If the distance between the tibia and the fibula is clearly greater, due to complete disruption of the syndesmosis, it is usually obvious on radiography, particularly on the mortise view [13, 25]. Simple radiography is also useful to rule out associated fractures [2, 9]. However, in some individuals, the diastasis is not as clear on radiographs, even with complete ligament ruptures; thus, this method of imagery will fail to detect syndesmotic injuries in about 35-50% [23, 25, 26]. Therefore, when there is no clear diastasis nor clinical examination findings, syndesmosis injuries can be hard to diagnose [8, 9, 27]. A CT scan is a more sensitive diagnostic tool for syndesmosis injuries [13, 23, 24, 28, 29]. When identified, pre- or intra-operatively, there are multiple treatment options described in the literature [16, 30]. Indeed, various surgical treatments are available to maintain or regain this stability, such as metallic screw fixation, absorbable screw, and dynamic suture button fixation devices [16]. In general, when mortise widening can be seen on imagery, surgical treatment with one of these devices is required [2]. However, if only one or two ligaments are ruptured and there is still some stability in the syndesmosis, conservative treatment can be the solution [2].
A previous study showed that the CAM (controlled ankle motion) boot could slightly increase external rotation of the fibula when axial loading was applied to the ankle, possibly because of the posterior cushions inside the boot [31]. Considering this, and knowing that no other study had evaluated this precise topic before [32], the following research question emerged: does “high-ankle sprain” taping have an impact on syndesmosis congruity under axial loading with different ligaments ruptured?
The main purpose of this study was to evaluate the effect of high-ankle sprain taping on syndesmotic stability in various ligament conditions when axial loading is applied. The hypothesis is that high-ankle taping will not modify the distal anatomy between the tibia and fibula in axial loading with a syndesmotic injury; more specifically, we believe there will be no overtightening of the distal tibia and fibula.
2. MATERIALS AND METHODS
The first steps of this study were the same as our previous study with the CAM orthopaedic boot [31]. Approval from the Institutional Review Board Committee was obtained. Unused fresh-frozen specimens were removed from the freezer around 24 to 30 hours before experimentation and dissected to expose the syndesmosis and tibial plateau. An antero-lateral approach was used to expose the syndesmosis.
A 3D-printed device to support the leg and apply axial loading was designed to support the heel and the tibial plateau. The neutral position of the ankle was maintained to simulate axial loading (AL). An Omegadyne load cell was set up between two parallel 12-inch fully threaded rods on the device. Each specimen was then positioned in the leg-holder and loaded with 750 N of force, simulating weight-bearing. The target of 750 N, which was modeled on several other cadaveric studies [1,4,33,34], is an estimate of the force representing the weight of an average person standing on his/her foot as the determined surface area (Fig. 1).

High-ankle sprain taping, or ring taping, was done by the same senior orthopaedic resident on each cadaver. He had previously learned the proper technique with a physiotherapist specialized in sports medicine and experienced in this method. Pre-taping underwrap (thin, lightweight foam) was rolled just above the malleolus. Rigid adhesive tape, used by the physical therapy department of our institution, helped compress the tibia and the fibula towards one another by wrapping it around the syndesmosis (Fig. 2).

First, images of the intact specimen, without axial loading, were taken. Pure axial loading was applied and a new series of images were taken. Finally, high-ankle sprain taping was added to the specimen before a new imaging sequence in the CT scan. After this baseline data was defined, the AiTFL was sectioned. Images were taken with and without axial loading, as well as with taping and AL. The whole sequence was repeated following the sectioning of the IOL, up to 10 cm proximally. The deltoid ligament was kept intact.
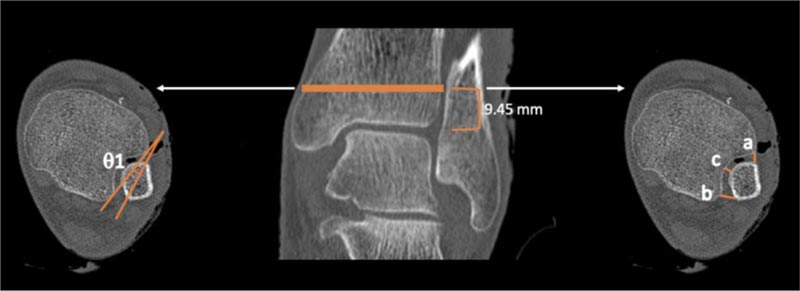
To evaluate the relationship between the distal tibia and fibula, a previously validated method composed of five measurements on CT scan was used [24]. More specifically, in this study, three-length measurements (a,b,c) and one angle (θ1) were recorded [24] (Fig. 3).
The length “a” is measured as the distance between the most anterior point of the incisura and the nearest most anterior point of the fibula. [ 24 ] Length “b” is determined by measuring the distance between the most posterior point of the incisura and the nearest most posterior point of the fibula. [ 24 ] Distance “c” is defined as the distance between the tibia and the fibula in the middle of the incisura. [ 24 ] Finally, Angle 1 represents the angle between a line drawn from the anterior and posterior point of the incisura and a line drawn in the fibula representing its orientation; according to these measurements, internal rotation is represented by a negative angle. [ 24 ] This method to evaluate the syndesmosis using CT scan images was also used in a similar study on the effect of controlled ankle motion walking boot on syndesmotic instability [ 31 ].
Measurements on all CT scan slices were taken by the same senior author.
Each specimen was compared, and data were analyzed using Wilcoxon tests for paired samples and non-parametric data, with SPSS statistics 25.0 (IBM). In order to control for the multiplicity of tests and considering the nature of this study (controlled experimental study), the level of significance was set at 0.01 for these analyses.
3. RESULTS
Ten paired cadaveric specimens from mid-thigh to toes were used for this study, including four males and one female. Their average age was 71 years old. All specimens underwent the full complement of testing and ligament rupture simulation. Although our specimens’ mean age was 71 years, we believe these results are applicable to all individuals because no significant degenerative changes seen on CT scan were present in the ankles we used. There were no significant differences when comparing the ankles with and without AL. This remained true for all specimens with isolated AiTFL “tears” and in those with both AiTFL and IOL “tears” (p<0.01, Table 1).
We also could not establish any significant effect of high-ankle sprain taping on syndesmotic stability, whether an isolated AiTFL or combined AiTFL and IOL ruptures were simulated, and this was true regardless of the axial loading state (Table 1).
4. DISCUSSION
The main purpose of this study was to evaluate the effect of high-ankle sprain taping on the stability of the tibiofibular syndesmosis in different conditions of simulated axial loading and ligament injury. Our hypothesis was that high-ankle sprain taping would not modify the relationship between the distal tibia and fibula.
| - | 1-Without AL | 2-With AL | 3-With AL + Ring Taping | p-value (1 vs. 2) | p-value (2 vs. 3) |
|---|---|---|---|---|---|
| a(mm) | - | - | - | - | - |
| Intact ankle | 3.68 (±1.00) | 4.05 (±1.11) | 4.19 (±1.03) | 0.046 | 0.258 |
| AiTFL | 3.85 (±1.24) | 4.06 (±1.14) | 4.02 (±1.06) | 0.612 | 1.000 |
| AiTFL+IOL | 4.46 (±0.87) | 4.31 (±0.68) | 4.28 (±0.92) | 0.122 | 0.959 |
| b(mm) | - | - | - | - | - |
| Intact ankle | 7.58 (±1.81) | 7.55 (±1.82) | 7.44 (±1.58) | 0.683 | 0.953 |
| AiTFL | 7.57 (±2.15) | 7.10 (±1.91) | 7.04 (±2.08) | 0.097 | 0.812 |
| AiTFL+IOL | 7.19 (±2.17) | 7.20 (±1.98) | 7.17 (±2.09) | 0.905 | 0.721 |
| c(mm) | - | - | - | - | - |
| Intact ankle | 2.01 (±0.47) | 2.09 (±0.39) | 2.02 (±0.41) | 0.371 | 0.440 |
| AiTFL | 1.98 (±0.55) | 2.06 (±0.61) | 2.19 (±0.48) | 0.622 | 0.338 |
| AiTFL+IOL | 2.06 (±0.64) | 2.12 (±0.57) | 2.28 (±0.51) | 0.509 | 0.056 |
| Angle 1(°) | - | - | - | - | - |
| Intact ankle | -8.31 (±6.54) | -7.98 (±5.76) | -9.03 (±5.68) | 0.575 | 0.236 |
| AiTFL | -6.76 (±5.59) | -7.80 (±5.82) | -7.33 (±6.14) | 0.046 | 0.610 |
| AiTFL+IOL | -6.08 (±4.23) | -7.27 (±5.00) | -6.86 (±5.46) | 0.038 | 0.959 |
According to our experimental values and the level of significance set to 0.01, no significant displacement of the fibula in relation to the tibia was noted, with or without the high-ankle sprain tape, in any ligament and loading combination. Therefore, it is impossible to accept or reject our hypothesis because there was no significant displacement when we compared ankles with and without AL.
The data for Angle 1 has a wide range. In intact ankles without AL, the difference is approximately 13 degrees, -8.31(±6.54), and with AL and both ligaments ruptured, the mean is -7.27 (±5.00). This wide range was also noted in a study by Patel et al. where they used the same measurement method as in this study. [ 37 ] Their mean for Angle 1 in weight-bearing ankles was -12.78 (5.45) with a range between -24.00 and 6.00 degrees [37].
The fact that no significant change was observed during this study could be explained in many ways. First, results might have been different if an external rotation force had been applied to the custom-made weight-bearing simulation device. External rotation is known to be a common injury mechanism when the syndesmosis is involved [35]. Indeed, a study conducted by Beumer et al. showed that external rotation is the force that causes the most significant displacement of the fibula at the syndesmosis level [36]. They also found that external rotation of the ankle-foot complex led to the rotation of the fibula, causing the narrowing of the syndesmosis width [36]. This may explain why AP radiography is not a good radiologic tool to assess syndesmosis instability [36]. Consistent with our results, they did not find the frank displacement of the fibula with regard to the tibia when the foot was placed in the neutral position, with or without axial loading, when the AiTFL, the PiTFL and the anterior part of the deltoid ligament were sectioned [36].
Second, the deltoid ligament is one of the ankle’s primary stabilizers [13]. It can be argued that significant displacement could have been caused by iatrogenic rupture of the deltoid ligament, as well as the full syndesmotic complex disruption. We chose not to do this because we believe that three ligament tears will have a visible diastasis and a clear surgical indication. However, two ligament injuries do not have a clear surgical indication, and therefore ankle taping may be of some benefit. Finally, cadaveric thawed tissue cannot adequately replicate in vivo conditions with live tissue.
In order to analyze the capacity of high-ankle sprain taping to maintain syndesmotic congruity, baseline displacement data on CT scan with axial loading was needed. Unfortunately, there was no significant difference in any measurement or angle among specimens, with and without axial loading. Isolated time-point axial loading in neutral position seems to have no significant effect on syndesmotic anatomy with two injured ligaments.
It is important to note that high-ankle sprain taping did not cause any malreduction of the distal tibiofibular joint. The same cannot be said for the CAM boot. In a previous study, Lamer et al. found that the CAM boot can increase external rotation of the fibula when AL is applied, which may interfere with proper healing [31]. In the present study, even when the syndesmosis was not intact and two ligaments were ruptured, putting on a ring tape did not change the anatomy of this joint. This might argue in favor of high-ankle sprain taping when treating certain types of syndesmotic injury.
Hunt et al.’s study demonstrated that axial loading alone, without external rotation, did not impact intraarticular contact pressure or syndesmosis stability [1]. No significant displacement and rotation of the fibula or talus greater than 0.5 mm and 1 degree were found in their study during AL alone without any rotation force [1].
These findings suggest that in the clinical setting, when an incomplete syndesmotic rupture is treated conservatively, the external rotation should be avoided, with taping, a CAM boot or a cast. There is no specific standardized rehabilitation program to allow proper ligament healing [12]. Immobilization and a progressive return to function are left to the discretion of the treating doctor and the rehabilitation team. Normally, this process would start with rest, ice and elevation, followed by a non-weight-bearing period [12, 13]. During this period, would high-ankle sprain taping be enough to restrain syndesmosis congruity even with an external rotation force applied? Further studies are needed to answer this question.
The main limitation of our study stems from its cadaveric design. Ligaments were sectioned but the other soft-tissue structures (such as the capsule and the deltoid ligament, among others) were not damaged, contrary to what is frequently found in real-life injuries. This could have provided the specimens with more stability than what is normally seen. Also, the specimens were only stressed with an axial load without rotational components, which, again, does not reproduce the pattern of true ankle injuries. Furthermore, dynamic loading, modeled more closely in real-life, could have revealed differences over time. This is a potential future research avenue. Finally, in a clinical setting, the relative tension applied to the ring tape can be adjusted based on patient feedback. In cadaveric specimens, since this is not possible, there is a potential for over-tensioning. Clearly, more studies are needed to evaluate the theoretical benefits and use of high-ankle sprain taping. This study is, to our knowledge, the first to assess radiographically the effect of high-ankle sprain taping on the tibiofibular syndesmosis in an axial loading setting.
CONCLUSION
It is impossible to conclude if high-ankle sprain taping can maintain syndesmotic congruity because we found no significant difference, even with AL and two ruptured ligaments, whether taping was used or not. However, this study confirms the hypothesis that high-ankle sprain taping does not cause a malreduction of the distal tibiofibular joint when one or two ligaments are torn in neutral weight-bearing condition. These results support its use as a conservative treatment for syndesmosis injury in strict axial loading condition without any external rotation. This is the first study evaluating the effect of high-ankle sprain taping and because there are no evidence-based guidelines regarding syndesmotic injury treatment, taping could become an interesting alternative. However, further studies to evaluate its function with cyclical dynamic axial loading, as well as external rotation force, would be needed.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethics committee approval was granted by the Comité d'éthique à la recherche CIUSSS NIM - Sacre-Coeur Hospital in Montreal, # CER 2015-1169.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
Not applicable.
AVAILABILITY OF DATA AND MATERIALS
The data that support the findings of this study are available upon request from the authors.
FUNDING
The authors report departmental funding to the institution for research and education purposes from Arthrex, Conmed, Depuy, Linvatec, Smith & Nephew, Stryker, Synthes, Tornier, Wright, Zimmer Biomet.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The authors wish to thank the PREMIER program for an educational grant and Kathleen Beaumont for manuscript review and preparation.

