All published articles of this journal are available on ScienceDirect.

Surfing Injuries in Norwegian Arctic Waters
Abstract
Objectives:
To investigate the frequency, types, mechanisms and treatments of acute surfing injuries in cold and arctic waters, and to compare the findings with studies of surfing injuries from warmer waters.
Materials and Methods:
Retrospective web-based survey relating to acute surfing injuries in Norway. An acute injury was defined as sudden onset, with a clearly defined cause or onset, and leading to an inability to surf for at least one day.
Results:
From the 974 respondents, 245 (25%) reported a total of 511 acute injuries. The injury rate was 2.2 injuries per 1000 surfing days (0.74 per 1000 surfing hours). Head/neck was the most commonly injured body part. Lacerations were the most frequently reported injury type. Trauma from contact with the surfboard was the most commonly reported injury mechanism. Wetsuit equipment was used by 99% of the respondents.
Conclusion:
Surfing in cold and arctic waters leads to different injuries compared with surfing in warmer waters. These differences may be attributed to the use of wetsuit equipment. Surfing in Norway is relatively safe, however, some severe head injuries were reported which may have been prevented by the use of a helmet.
INTRODUCTION
Wave surfing in Norway has existed since the 1980s, and has grown rapidly in popularity. Along the 28,953km Norwegian coastline, there are numerous surf spots; from the south-eastern coast and up as far as 70° north. The best known and most frequently surfed spots are in the south-western region of Jæren close to the city of Stavanger, the Stad Peninsula on the north-western coast of southern Norway, and the Lofoten Islands in northern Norway [1]. In these surf spots there are surf schools and surf shops with surf equipment rental possibilities.
The climate in Norway can be cold, and the northern part of the country has an arctic climate with air temperatures down to -20°C and water temperature around the freezing point in the winter. Little is known about surfing injuries in cold climates and waters. Several studies on surfing injuries in warmer climates of the world have been conducted, including Australia, Brazil, Hawaii, USA, Tahiti and Argentina [2-5]. These studies have found a dominance of lacerations/abrasions or sprains/strains, with the lower limbs and head being the most frequently injured sites. The most severe injuries found in these studies were to the head and spine.
While surfing in cold waters, there is a risk of hypothermia. As mentioned by the authors of the book Surf Survival [6], wetsuits should be viewed as important pieces of the surfing gear. While the primary purpose is to keep a surfer warm, it also provides excellent sun protection, significant floatation, and some protection against abrasions from the seafloor.
The aim of this study is to investigate the frequency, types, mechanisms and treatments of acute surfing injuries in cold and arctic waters, and to compare these findings to the studies of surfing injuries in warmer parts of the world. Can the wetsuit protect the cold water surfer from other typical surf injuries as well? Is there a difference in acquired surf injuries in warm water and cold water because of the wetsuit used in cold water? Or will the cold water surfer be more prone to get muscle strains and sprains because of muscle tremors [7] and cold stiff muscle fibers?
MATERIALS AND METHODS
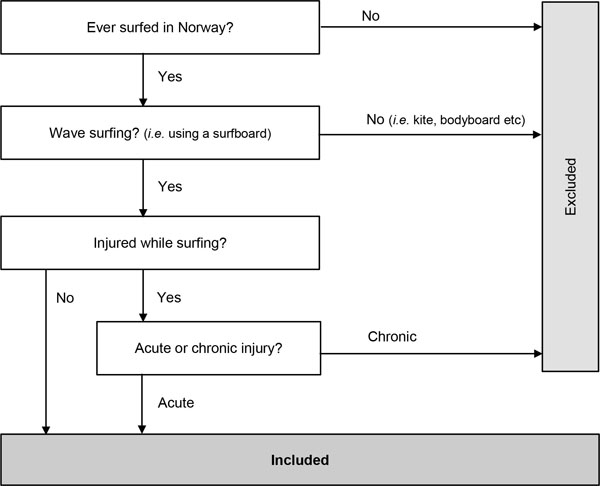
In this study ‘surfers’ were defined as participants in wave surfing using a surfboard, excluding kite surfers, wind surfers, kayak surfers and bodyboard surfers. Included were surfers that had wave surfed in Norway, regardless of citizenship or country of residence. The definitions of the eligible participants and characteristics are summarized in a flow chart in Fig. (1).
Data were collected with a web-based questionnaire. The questionnaire retrieved information about gender, age, citizenship, surfing frequency, equipment, environmental factors and acute surfing injuries. The respondents were asked to describe the site of the injury, the injury type, the cause of the injury and any treatment received. In order to calculate the injury rate of acute surfing injuries, both injured and non-injured surfers were included in the survey results. An acute injury was defined as a sudden onset injury, with a clearly defined cause or onset [8], leading to an inability to surf for at least one day. The respondents were asked to recall injury details from their entire surfing experience in Norway. Surfers entered the survey voluntarily and could choose to answer anonymously. The respondents could exit the survey at any time.
The questionnaire was developed and validated by the investigators using the professional version of the online survey tool Survey Monkey, (Gold version 2013, manufactured by SurveyMonkey Inc). The questionnaire was located at the website: www.surveymonkey.com/s/CZMQX9R. Data collection was carried out between March 2013 and June 2013. Invitations to participate in the survey were distributed on several surfing-related websites such as websites for surf schools, surf clubs, surf camps, surf magazines and surf contests. Many of these were Facebook websites. Personal invitations were also sent to members of different surfing-related Facebook groups. These groups had diverse geographical and surfing-related origins. The websites were mostly Norwegian and Swedish. Both the invitations and the questionnaire were in English as well as Norwegian. Information about the survey was also given directly to surfers by the main author.
Information about the use of the data, and that the data would be treated with confidentiality and privacy according to the Norwegian Data Protection Authority privacy regulations, was given to the respondents. Respondents under the age of 18 years were asked to provide consent from a parent before completing the questionnaire. The study was approved by the Regional Committee of Ethics in Medical Research (Mid Norway).
Data were analyzed with the IBM SPSS Statistics version 20 software for Mac. The analysis applied with the SPSS was descriptive statistics; frequencies, descriptives and cross tabulations. Only data from respondents that had completed the main part of the questionnaire were included in the analysis.
RESULTS
Surfing Demography
The survey had a total of 1049 responses: 75 responses (7%) were excluded; 25% had not surfed in Norway, and 75% had not completed the main part of the questionnaire or answered the questions.
A total of 974 respondents were included in the study. The mean age of the respondents was 29 years (range 12-60 years). The number of male respondents was 696 (71%). Surfers from 28 different countries were included: 817 (84%) were from Norway.
Mean surfing experience was six years (range 1-32 years), 29 days per year (range 0.5-285 days) and 3.4 hours per surfing day (range 1-8 hours).
Four-hundred and nine (42%) of the respondents surfed most often in fall/winter from October to March, possibly due to better wave conditions, 304 (31%) surfed most often in spring/summer from April to September and 261 (27%) surfed just as frequently in fall/winter as in spring/summer.
Three-hundred and forty respondents (35%) surfed most frequently in south-western Norway, 338 (35%) in mid-western Norway, 175 (18%) in northern Norway and 111 (11%) surfed most of the time in south-eastern Norway.
Four-hundred and eighty-three (50%) surfed most frequently over hard seafloor, that is, rocks or a mix of sand and rocks. Six-hundred and one (62%) surfed most often in waves over one meter high. Five-hundred and ninety-seven (61%) surfed most of the time on a shortboard and 357 (37%) on a longboard. Concerning safety protection equipment, 972 (99%) used wetsuits, 899 (92%) used shoes, 816 (83%) used gloves and 801 (82%) used a hood. Hoods, gloves and shoes for surfing are usually made of neoprene. Forty-five (5%) used a nose guard (a protective guard made of rubber, placed on the sharp front tip/nose of the surfboard to prevent penetrating injuries), and 34 (4%) used earplugs. Ten (1%) of the respondents reported occasional use of a helmet, which was used primarily when surfing over hard seafloor, in shallow water, or when surfing alone in big waves. Wetsuit heating systems were used by 6 (0.6%) of the respondents.
Injury Frequency
Five-hundred and eighteen injuries were reported, seven of these injuries were excluded because they were not acute leaving a total of 511 acute surfing injuries included in the study. These injuries were reported by 245 (25%) of the respondents which equates to a mean of 2.1 injuries (range 1-24) per surfer. The injury rate was 2.2 per 1000 surfing days, and 0.74 per 1000 surfing hours. Details were provided for 421 of the injuries.
Injured Body Part
Out of the 421 injuries, 182 (43%) injuries were to the head/neck and 121 (29%) to the lower limbs. Sixty-three (15%) of the injuries were to the upper limbs, and 54 (13%) were to the torso.
Injuries to the head/neck were most commonly to the skull 88 (48%) or face 41 (23%). Lower limbs injuries were most commonly to the foot 30 (25%) or knee 27 (22%). The most common upper limb injuries were to the shoulder 27 (43%) or hand 19 (30%), and the torso injuries were most commonly to the back 33 (61%) or chest/ribs 19 (35%).
Type of Injury
The most frequently reported injury types were lacerations/abrasions 128 (30%), contusions 89 (21%), sprains/strains 88 (21%), fractures 42 (10%) and concussions 27 (6%). Together these types accounted for 374 (89%) of the total 421 described injury types. In twelve cases (3%), injuries related to hypothermia were reported.
Lacerations/abrasions to the head/neck were the most frequently reported injuries, secondly came sprains/strains to the lower limbs (Table 1).
| Head/neck | Lower limbs | Upper limbs | Torso | Other | Total | ||
|---|---|---|---|---|---|---|---|
| Laceration/ abrasion |
n | 88 | 30 | 8 | 2 | 0 | 128 |
| % | 20.9% | 7.1% | 1.9% | 0.5% | 0% | 30.4% | |
| Contusion | n | 28 | 28 | 12 | 21 | 0 | 89 |
| % | 6.6% | 6.6% | 2.9% | 5.0% | 0% | 21.1% | |
| Sprain/ strain |
n | 5 | 46 | 26 | 11 | 0 | 88 |
| % | 1.2% | 10.9% | 6.2% | 2.6% | 0% | 20.9% | |
| Fracture | n | 14 | 6 | 7 | 15 | 0 | 42 |
| % | 3.3% | 1.4% | 1.7% | 3.6% | 0% | 10.0% | |
| Dislocation | n | 0 | 3 | 6 | 0 | 0 | 9 |
| % | 0% | 0.7% | 1.4% | 0% | 0% | 2.1% | |
| Other* | n | 47 | 8 | 4 | 5 | 1 | 65 |
| % | 11.2% | 1.9% | 1.0% | 1.2% | 0.2% | 15.4% | |
| Total | n | 182 | 121 | 63 | 54 | 1 | 421 |
| % | 43.2% | 28.7% | 15.0% | 12.8% | 0.2% | 100% | |
Cause of Injury
Trauma from contact with the surfboard was the most common cause of injury resulting in 196 (47%) of all the described injuries.
One-hundred and three (25%) injuries were due to traumatic contact with the seafloor, and 60 (14%) were injured in connection with surfing maneuvers.
Out of the total injuries caused by the surfboard; 155 (79%) were from contact with the surfer’s own board, 35 (18%) from contact with another surfer’s board, five (3%) from the surfer’s own leash and one (0.5%) from another surfer’s leash. Seventeen (4%) respondents reported low temperature and climate as a cause of injury.
Lacerations/abrasions caused by contact with the surfboard were the most frequently described injury type and mechanism. Secondly were sprains/strains sustained due to surfing maneuvers (Table 2).
| Surfboard | Seafloor | Maneuvers | Wave force | Climate | Other | Total | ||
|---|---|---|---|---|---|---|---|---|
| Laceration/ abrasion |
n | 92 | 28 | 2 | 3 | 0 | 3 | 128 |
| % | 21.9% | 6.7% | 0.5% | 0.7% | 0% | 0.7% | 30.4% | |
| Contusion | n | 43 | 36 | 3 | 6 | 0 | 1 | 89 |
| % | 10.2% | 8.6% | 0.7% | 1.4% | 0% | 0.2% | 21.1% | |
| Sprain/ strain |
n | 14 | 13 | 46 | 8 | 4 | 3 | 88 |
| % | 3.3% | 3.1% | 10.9% | 1.9% | 1.0% | 0.7% | 20.9% | |
| Fracture | n | 24 | 11 | 2 | 3 | 0 | 2 | 42 |
| % | 5.7% | 2.6% | 0.5% | 0.7% | 0% | 0.5% | 10.0% | |
| Dislocation | n | 1 | 1 | 3 | 4 | 0 | 0 | 9 |
| % | 0.2% | 0.2% | 0.7% | 1.0% | 0% | 0% | 2.1% | |
| Other* | n | 22 | 14 | 4 | 10 | 12 | 3 | 65 |
| % | 5.2% | 3.3% | 1.0% | 2.4% | 2.9% | 0.7% | 15.4% | |
| Total | n | 196 | 103 | 60 | 34 | 16 | 12 | 421 |
| % | 46.5% | 24.5% | 14.3% | 8.1% | 3.8% | 2.9% | 100% | |
The most common surfing injury found in this study, was laceration/abrasion injuries to the head/neck, caused by traumatic contact with the surfer’s own surfboard.
Treatment
Medical help was sought for 164 (39%) of the reported injuries: 137 (33%) from an Emergency department or a general practitioner, 18 (4%) needed day treatment at a hospital and nine (2%) were hospitalized. Out of the nine injuries that led to hospitalization, four (44%) were head injuries; three (33%) were concussions with syncope caused by contact with the seafloor, and one (11%) was a skull fracture after contact with the surfboard.
Injury Trends
Twenty-nine percent of the male and 16% of the female respondents had been injured. Thirty-two percent of those who most often used a shortboard, and 15% of those who preferred longboards had been injured. Thirty-five percent of the injured respondents surfed most often over a hard seafloor, compared to 16% that surfed mostly over a sand seafloor. Thirty-six percent of the winter/fall surfers and 11% of the summer/spring surfers had been injured. Thirty-nine percent of the respondents that surfed most often in waves over one meter high reported injuries compared with only 15% among those surfing in waves under one meter high.
DISCUSSION
The main finding in this study was an acute injury rate of 2.2 per 1000 surfing days, and 0.74 per 1000 surfing hours. This injury rate is therefore among the lowest reported. Injury rates in other surfing injury studies ranged from 2.2 to 3.5 injuries per 1000 surfing days, and 1.1 to 6.6 injuries per 1000 surfing hours [2-5].
Cold Surfing Injuries vs. Warm Surfing Injuries
The results of the present study compared to other studies on surfing injuries conducted in warmer parts of the world are summarized in Table 3.
| Study | Lowdon [2] | Steinman [3] | Nathanson [4] | Taylor [5] | Present study |
|---|---|---|---|---|---|
| Population and geographic origin |
Retrospective survey of 346 members of Australian Surfing Association, Victoria, Australia. | Retrospective survey of 930 surfers in Brazil. |
Prospective study of surfers in 32 competitions in Hawaii, Australia, California, Tahiti and Argentina. |
Prospective survey of a convenience sample of 646 surfers interviewed at beaches in Victoria, Australia. | Retrospective survey of 974 people who have surfed in Norway. |
| Average age (SD) | 22 (5.7) | 24 (6.3) | 24 (7) | 28 (7.9) | 29 (7.3) |
| Male gender | 95% | 95% | 87% | 90% | 71% |
| Average of years surfing | 8 | 59% > 5 years | Unknown | 12 | 6 |
| No. of acute injury | 311 | 766 | 116 | 168 | 511 |
| Injury rate Injuries/ 1000 d |
3.5 | 2.5 | - | 2.2 | 2.2 |
| Injuries/ 1000 h | 1.2 | 6.6 | 1.1 | 0.74 | |
| Injured body part Head/neck |
37% | 16% | 25% | 29% | 43% |
| Lower limbs | 63% | 38% | 39% | 46% | 29% |
| Upper limbs | 18% | 25% | 5% | 15% | |
| Torso | 8% | 11% | 20% | 13% | |
| Other | 0% | 21% | 0% | 0.2% | |
| Type of injury Laceration/abrasion |
44% | 53% | 35% | 46% | 30% |
| Contusions | 4% | 20% | 9% | 0% | 22% |
| Sprain/strains | 29% | 19% | 39% | 29% | 21% |
| Fractures | 16% | 3% | 5% | 9% | 10% |
| Dislocations | 1% | 4% | 4% | 11% | 2% |
| Other* | 6% | 2% | 9% | 5% | 14% |
| * Includes tympanic membrane rupture, tooth fracture/avulsion, concussion, hypothermia and near drowning. | |||||
| Cause of injury Surfboard |
53% | 36% | 29% | 42% | 47% |
| Seafloor | 13% | 17% | 24% | 18% | 25% |
| Wave force | 6% | 12% | 36% | 8% | |
| Surf maneuver | 17% | 35% | 16% | 0% | 14% |
| Marine animal | 1% | 9% | 2% | 1% | 0.3% |
| Other | 10% | 3% | 17% | 3% | 6% |
In the present study the head/neck were the most frequent injured body part, followed by the lower limbs. In other studies of surfer injuries the lower limbs were the most frequently injured part of the body (ranging from 38% to 46%), with head/neck being second (ranging from 16% to 37%) [2-5]. The present study found a lower amount of lacerations/abrasions compared to the studies from warmer climates, but a higher number of contusions. The widespread use of wetsuits and shoes among surfers in Norway, may explain the differences as the neoprene possibly protects the surfer from laceration/abrasion injuries to the lower limbs.
Surfers in warmer climates often only wear boardshorts. For the same reason contusions might be reported relatively more frequently.
The finding of lacerations/abrasions being the most often sustained type of injury was similar in both the present study and most other studies. The exception being the Nathanson et al. study which found strains/sprains were the most frequent injury type [4]. The present study had fewer sprains/strains than the Nathanson et al. study, and fewer dislocations than three of the comparable warmer-water studies [3-5]. This may again be explained by the use of a tight wetsuit which limits joint range of motion.
Unsurprisingly, hypothermia-related problems were reported more frequently in the present study. Three percent of the injuries were reported as either hypothermia or frostbite, and a total of 4% of the injuries were reported as occurring because of the cold climate or low temperature. In the Steinman et al. study, 0.4% of the injuries were related to hypothermia [3]. Improved wetsuit technology has made it possible to surf in relative comfort over an extended period of time even in the icy-cold waters of the far north and far south. However, one’s ability to produce and conserve heat will eventually be overtaken by the rate of loss of heat to the cold environment. This results in a slowing of the heart rate, lower blood pressure, impaired decision-making capacity, and muscle weakness. Hypothermia has been implicated as a contributing factor in numerous drowning deaths among cold-water surfers [6]. So far there is only one report of surfing-related fatalities in Norway.
The present study found a higher incidence of concussions (6.6% compared to 3% in the Taylor study [5]). Concussion injuries can be especially dangerous if the surfer loses consciousness in water.
Trauma from contact with the surfboard was the most often reported injury mechanism, both in the present study and the studies we compared to.
As suggested by Taylor et al. [10], rubber guards on the surfboards nose and soft-edged or rubber-guarded fins may help reduce the number of lacerations without altering surfboard dynamics. In a study by Nathanson et al. [11], 40% of surfers reported using nose guards and 5% of the surfers used soft-edged fins. Only 4.6% of the respondents in the present study used nose guards. In this study, they were not asked about the use of soft-edged fins. An Australian study found that a nose guard provides a 29-80% reduction in the impact delivered by the nose of a surfboard [12]. We are not able to explain why injuries due to contact with the seafloor were found to be more frequent in the present study.
In the present study the severe injuries that needed hospitalization, were mostly head injuries. Injuries to the head and/or spine were also reported as the most severe injuries in other studies [2-5, 9]. In a study by Taylor et al. [13], 2% reported routine use of headgear, and 10% used it occasionally. In the present study only 1% reported occasional helmet use.
Surfing in the winter months with shortboards over hard seafloor and in waves higher than one meter increased the risk of getting injured. Similar patterns were found by Nathanson et al. [4] In that study, the adjusted risk of injury was 2.4 (95% CI 1.5-3.9) times greater when surfing in waves overhead or bigger, compared with surfing in waves less than overhead, and 2.6 (95% CI 1.3-5.2) times greater when surfing over a rock or reef bottom compared with a sandy bottom.
In the present study there was a higher proportion of female surfers (29%) compared to the other studies. In the Lowdon study [2] from 1983 there were only 5% female respondents.
Main differences between cold surfing injuries in the present study and warm surfing injuries in the studies we compared to, are summarized in Fig. (2).

Injury Rates in Surfing vs. Other Sports
Compared to another water sport such as kite surfing which has an injury rate of 7 injuries per 1000 kiting hours [14], the injury rate in the present study is relatively low. Compared to winter sports such as snowboarding with 4 injuries per 1000 skier days, alpine skiing with 1.2 injuries per 1000 skier days and telemark skiing with 0.9 injuries per 1000 skier days [15], the injury rate in the present study is in the same range. Some of the most popular sports in Norway is soccer and handball, lower division soccer has an injury rate of 13 per 1000 played hours [16] and handball with 2.5 injuries per 1000 played hours [17]. Compared to the injury rate in soccer, the injury rate in surfing is very low.
Study Limitations
A limitation of the study could be difficulties for the surfers to recall details of all their injuries. Another limitation of the study might be the sampling strategy. Most of the information and invitations to participate in the study were distributed through surfing related Facebook-groups and other surfing related web sites, which may not be a representative sample of the total surfing population in Norway. As this descriptive data is not population based, the results must be read accordingly.
Internet-based online surveys have been conducted by other studies on surfing injuries, and response rates and injury descriptions were similar [11, 18].
Injury Prevention and Future Research
This study provides a general overview of acute surfing injuries and injury patterns in cold waters, which may lead to a better knowledge of injury prevention and treatment of surfing injuries. Due to the finding that the most frequently injured parts of the body were the head/neck, and that the most severe injuries were to the head, the use of surfing helmets is recommended, especially when surfing over hard seafloor and/or in big waves. Nose guards on the tip of the surfboard and soft edged fins may help reduce the risk of lacerations. Earplugs and/or neoprene caps would protect surfers’ ears, and may reduce the likelihood of tympanic membrane rupture [19].
This study only looked at acute surfing injuries. Little is known about chronic surfing injuries in cold water. Likewise little is known about helmet use and surfing, would more widespread use of helmets minimize severe head injuries in surfing?
CONCLUSION
The injury rate from surfing in Norway was found to be 2.2 injuries per 1000 surfing days. The most commonly injured parts of the body were the head/neck. Lacerations/abrasions were the most frequently reported injury types, and contact with the surfboard was the main mechanism of injury. The differences between surfing injuries in cold and arctic waters and warmer waters, may be due to the widespread use of wetsuit equipment. Surfing cold and arctic waters seems to be relatively safe, however, some severe head injuries were reported which might have been prevented by the use of a helmet.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
Thorlene Egerton, PT, PhD, at the Department of Neuroscience NTNU for the comments and help with language editing.
Børge Lillebo MD, at the Department of Neuroscience NTNU for help with the online survey tools.
Kristian Juberg, for the help with the figures.

