All published articles of this journal are available on ScienceDirect.

Highlighting Rural Cricket: Prevalence, Aetiology, and Risk Factors of Injury among Cricket Players in a Community Setting
Abstract
Objective:
Cricket is a bat-and-ball game played among teams. The game is correlated with complex proficiencies and strategies that require remarkable physical fitness levels. Investigations on competitive cricketers based on the community level are scanty. Furthermore, injuries occurring during play at this level are not well understood and additional research is required for injury prevention. The study explored the prevalence, aetiology, and risk factors of cricket injuries (sustained over a single season) among cricketers in a community setting.
Methods:
An epidemiological cross-sectional quantitative study design was performed. Data were collected from participants (n = 96), based on two cricket boards. A self-reported questionnaire for a single season was administered, which focused on demographics, the prevalence of injury, risk factors, and aetiology of injury.
Results:
A total of eighty-seven participants (90.6%) experienced injury or related musculoskeletal pain (K-S 0.145, p < 0.000). The most common sites were the upper limbs (51%), followed by the lower limbs (45.8). Specific anatomical sites prevalent were the shoulder (33.3%), ankle (33.3%), hand (25%), and thigh (22.9%). Overuse injuries (45.8%) were prevalent, as well as sprains (49%), strains (41.7%), and bruising (49%). Mechanisms included overuse (51%), rapid rotation (44.8%), and struck by ball (41.7%). Majority (82.3%) of the participants reported not having access to primary healthcare in the clubs.
Conclusion:
Community cricket players have a high overuse injury rate, concentrated mainly in the shoulder. Prevention and early primary healthcare are crucial in community-level sports.
1. INTRODUCTION
Cricket is a bat-and-ball game played in teams [1]. Cricket is considered a non-contact low-injury risk sport compared to other sports [2]. It is a multidimensional sport in which participants perform a wide range of activities such as batting, bowling, fielding (catching and throwing), and wicketkeeping [3]. Injuries and musculoskeletal pain can occur in all sporting activities [4]. Repetitive/overuse and acute traumatic (impact injury) injuries are the two most common types of injury mechanisms, with 64/100 players injured per season [5]. Methods of injury in cricket include acute trauma (hit by the ball, collision with players), overuse, rapid rotation motion, and medical illness [3]. Acute injuries are mostly correlated with ball strikes, and overuse injuries are associated with workload and repetitive motion [6].
Injury data from competitive cricketer settings do not apply to community-level cricket due to the differences in intensity, physiological adaptation, and risk factors [6, 7]. Engagement in community-level cricket is based on social factors, physical fitness, and sport enjoyment, indicating low intensity compared to competitive cricket. Some players are not physically adapted to engage in cricket (muscle endurance, muscle strength, flexibility, and agility) [8]. International and local studies focus mainly on injuries sustained by competitive cricketers. These studies indicate that upper limb injuries are more prevalent than lower limbs, with overuse as the main mechanism [4, 9]. Shoulder and hamstring injuries occur most frequently, especially in fast bowlers [5, 6]. Fielding was associated with hand injuries as evident in the rate of ball-strike related injuries [10].
Synergistically, both extrinsic and intrinsic risk factors predispose one to injuries in sports. Extrinsic factors include workload (number of overs bowled), player position, weather, and time of play. Intrinsic risk factors include physical fitness (muscular strength, flexibility, balance, and biomechanics), postural defects, and bowling/batting technique [2, 8, 11]. Community level players lack adequate training, physiological adaptation, and proper equipment. Hence, they are more prone to upper extremity overuse problems related to repeated ball throwing as well as muscle damage and strain, especially if there is insufficient rest for recovery. Furthermore, community level injuries often go undetected and untreated [12] and may only surface during game time, being severe enough to warrant medical attention. According to Russell, Hughes, Heskin, and Lee [10] prevention is crucial at the earliest stage. In contrast, studies related to elite cricket reveal that most injuries are related to direct blows and are treated early without the need for medical intervention [7].
Cricket is associated with a complex interplay between skills, strategy, and physical fitness [7]. Studies on competitive cricketers were more compared to community level cricket [13]. Cricket injuries at the community level are not well understood. Research is required into the prevalence rate, aetiology, and risk factors for timely prevention [7]. There is a dearth of information on the prevalence of injuries sustained by community club cricketers. Therefore, this study investigated the injuries sustained in community cricket about the prevalence, aetiology, risk factors, and medical attention received.
2. METHODS
2.1. Study Design
An epidemiological cross-sectional quantitative study design was adopted to determine the prevalence, aetiology, and risk factors of injuries among cricket players in a community setting. Participants (n = 96) were community-based cricket players aged 18 - 45 yrs and were recruited from two major community-based cricket unions/boards in Johannesburg, South Africa (Easterns Cricket Union and the Gauteng Lions Cricket Union).
Informed consent was obtained from all the participants and data collected during the study were kept strictly confidential. The study has conformed with the Helsinki Declaration and ethical approval was sought from the Faculty of Health Science Research Ethics Committee (REC-775-2020) at the University of Johannesburg, South Africa.
2.2. Study Procedure
Data were collected during a single cricket season (2019/2020), via a self-reported questionnaire (adapted from Noorbhai, Essack, Thwala, Ellapen and Van Heerden [8]). The questionnaires were administered online to participants and accompanied by a detailed explanation to reduce bias. The questionnaire consisted of four sections: (A) demographics: gender, age, race, occupation, and playing experience; (B) playing position and injury: occurrence, mechanisms, and prevention; (C) risk factors associated with cricket injuries, time of training, physical activity, intensity rate, and cricket formats; (D) evaluating the aetiology (causes of injury): has the participant sustained any injury, how, where, symptoms (pain), pain scale, healthcare service received. Open-ended questions were used to ascertain the effects of injury in play and injuries sustained for 5 yrs. An inductive content analysis approach was used for the free text responses to identify themes that could be utilized as categories in subsequent content analysis. Participants' responses were divided into clauses, with each clause categorized according to the themes that emerged.
In the absence of a medical certificate and medical practitioner participation, it was deemed unlikely that the prevalence and recall of injuries reported would be reliable. Participants would have not kept records of all the injuries sustained during the 2019/2020 cricket season. Nevertheless, for the purpose of this study, participants, the recall was deemed to be reliable in identifying the type of injury, type of symptoms, pain persistence, anatomical site, and aetiology.
2.3. Data Analysis
The data collected were coded with a distinctive player identity, imported into a Microsoft Excel (2016) dataset for preliminary editing, and then analysed with IBM SPSS Statistics for Windows (Version 25.0. Armonk, NY: IBM Corp.). The data were analysed using mean, mode, frequency, and percentages; for clarity, frequency and percentages were used in reporting the results. An independent T-test was performed to compare the means between the groups. The significance value was set at p ≤ 0.05.
The Levene test is a hypothesis test used to check if the variances of two or more groups are equal. It was used as a preliminary test before performing the t-test to ensure that the assumption of equal variances was not violated. The Levene test works by comparing the absolute deviations of each observation from the group mean and then testing whether these deviations are significantly different between the groups.
Similarly, KS test is a nonparametric test used to compare the distribution of the two samples. It was used to test whether the samples come from the same distribution or not. The KS test works by calculating the maximum difference between the cumulative distribution functions of the two samples and comparing it to a critical value based on the sample size and the desired level of significance. Therefore, the Levene test was applied to test for differences in variances between groups, while the KS test was to test for differences in distributions between the groups. Both tests are important tools in statistical analysis and can provide valuable insights into the data being analyzed.
3. RESULTS
Ninety-six (n = 96) participants partook in the study. Their ages ranged between 18 and 45 yrs. The mean age was 27.98 (SD 6.910) (Kolmogorov-Smirnova = 0.145, p ≤ 0.000. The assumption of homogeneity of variances (equal variance not assumed) with Levene’s F test revealed f = 0.715, p = 0.400. Afterward, the independent sample T-test was associated with a statistical significant effect (df = 93.794; T = 1.264, p = 0.204).
In South Africa, cricket is a male-dominated sport; hence 87 (90.6%) of the participants were males, and only 8 (8.3%) were females. Undisclosed gender was 1 (1.0%). In terms of ‘racial’ classification, a majority, 86 (89.6%) were blacks, 6 (6.3%) were colored, only 2 (2.1%) and 1 (1.0%) were Indians and Whites, respectively; with 1 (1.0%) of the respondents not selecting a race. Out of the 96 participants, 44 (45.8%) were employed, 22 (22.9%) had no occupation, and 30 (31.3%) did not respond.
Table 1 reveals the following results concerning risk factors: the majority of participants, 93 (96.9%), reported no risk factors, while 3 (3.1%) did. The latter group comprised of males, above 45 yrs or females 55 yrs. A family history of CVD, for example, heart failure/diabetes, was reported by 26 (27.1%), while the remaining 70 (72.9%) reported none; 4 (4.2%) of the respondents agreed that they have hypertension, while the remaining 92 (95.8%) did not. A total of 85 (88,5%) participants agreed that they were overweight/obese and 11 (11.5%) did not; 19 (19.8%) smoked cigarettes, while 77 (80.2%) did not; 36 (37.5%) exercised at least three times a week for 30 mins minimum, while the other 60 (62.5%) did not. Two (2.1%) participants had been diagnosed with dyslipidaemia/high cholesterol, while 94 (97.9%) were not; 7 (7.3%) had underlying conditions such as asthma, chronic obstructive pulmonary disease (COPD), liver disease, lung disease or cancer, but 89 (92.7%) do not; and 32 (33.3%) had none of the above risk factors while 64 (66.7%) had some of the above risk factors.
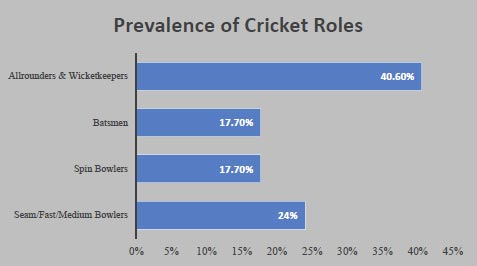
Fifty-four (56.3%) respondents had participated in the junior or senior provincial/national teams, while 42 (43.8%) had not competed in any of the levels. In terms of playing experience, 50 (52.1%) indicated having 5 – 10 yrs; 13 (13.5%) had 10 – 15 yrs; 26 (27.1%) had 0 – 5 yrs, and 7 (7.3%) more than 15 yrs. Playing positions of the participants revealed that all-rounder and wicketkeeper (39; 40.6%) were the dominants, followed by seam/fast/medium bowlers (23; 24%); then spin bowlers and batsmen with 17 (17.7%), respectively (Fig. 1).
| Variables | Response [n (%)] | |
|---|---|---|
| No | Yes | |
| Male and above 45 yrs or female and above 55 yrs | 93 (96.9%) | 3 (3.1%) |
| Family history of CVD; for example, heart failure/diabetes | 70 (72.9%) | 26 (27.1%) |
| I have hypertension (high blood pressure) | 92 (95.8%) | 4 (4.2%) |
| I am currently overweight/obese (BMI > 25 kg/m2) | 85 (88.5%) | 11 (11.5%) |
| I smoke cigarettes | 77 (80.2%) | 19 (19.8%) |
| Exercise at least 3 times a week for 30 mins minimum | 60 (62.5%) | 36 (37.5%) |
| I have been diagnosed with dyslipidaemia/high cholesterol | 94 (97.9%) | 2 (2.1%) |
| I have the following underlying conditions; for example, asthma, COPD, liver disease, lung disease, or cancer. | 89 (92.7%) | 7 (7.3%) |
| None of the above. | 64 (66.7%) | 32 (33.3%) |
*Note: All values are in actual percentage.
Majority (90.6%) of the participants reported having an injury or related musculoskeletal pain in the season 2019/2020. Upper limb (51%) was prevalent, followed by the lower limb (45.8%). The least [3 (3.1%)] was the head and neck region (Table 2). The most common type of injuries was overuse [44 (45.8%)], traumatic [29 (30.2%)], and a combination of both traumatic and overuse [23 (24%)]. Traumatic injury is caused by a single incident that causes an acute injury, whereas overuse is a repetitive or chronic injury that lasts over some period [8]. The types of injuries reported were: sprain 47 (49%), bruising 46 (47.9%), strain 40 (41.7%), open wound 12 (12.5%), and fractures with 5 (5.2%).
Basic sport-safe equipment is a prime necessity in all sports. In response to the provision responsibility of protective equipment, the study revealed that 49 (51%) of the participants indicated that it is an individual responsibility, and 33 (34.1%) indicated that it is both individual and teams’ responsibility. Only 14 (14.6%) believed it was the teams’ responsibility.
The following cricket practice frequencies of the participants in a year were: 42 (43.8%) five months, 26 (27.1%) six months, 9 (9.4%) seven months, 7 (7.3%) four months, 6 (6.3%) eight months, four (4.2%) three months, while only 2 (2.1%) practised for ten months. Similarly, the findings revealed 51 (53.1%) and 27 (28.1%) practices three and four times a week, respectively. Nine (9.4%) indicated training two times a week, and another nine (9.4%) indicated practising five times a week. Duration of practice per session in hours revealed: 68 (70.8%) for 3 hours, 23 (24%) for 2 hours, and only 5 (5.2%) for 4 hours. Similarly, forty-four (45.8%) of the participants indicated participating in activities additional to cricket practice, while 52 (54.2%) did not practice any other sport. Regarding the type of training activity participants engaged in weight training [6 (6.3%)]; aerobic [13 (13.5%)]; flexibility [1 (1%)]; agility [13 (13.5%)]; core-stabilization [1 (1%)]; cricket specific skills practice [4 (4.2%)] and others [58 (60.4%)]. The results further indicated that the exercises were conducted on the Borg Rating of Perceived Exertion (RPE) scale of 5 [11 (11.5%)]; 6 [29 (30.2%)]; 7 [32 (33.3%)]; 8 [16 (16.7%)]; 9 [7 (7.3%)] and 10 [1 (1%)].
The commonest game formats reported were fifty overs [73 (76%)]; twenty overs [40 (41.7%)], and forty overs [22 (22.9%)]; thirty overs [2 (2.1%)] and others [19 (19.8%)]. The type of pitch surface was predominantly grass [51 (53.1%); concrete [40 (41.7%)]; artificial turf [2 (2.1%)] and others [9 (9.4%)]. The study findings revealed that 75 (78.1%) have sustained injuries/pain in the last 12 months of participation; 12 (12.5%) indicated not sure of any injury and 9 (9.4%) reported being injury-free. Furthermore, 66 (68.8%) indicated that the injuries occurred during match play training sessions [55 (57.3%)] and other physical activities [30 (31.3%). Similarly, the injury’s mechanisms were mostly overuse injuries [49 (51%)]; rapid rotation movement [43 (44.8%)]; hit by the ball [40 (41.7%)]; struck by the bat [12 (12.5%)], collision [8 (8.3%)] and other means [11 (11.5%)] (Table 3).
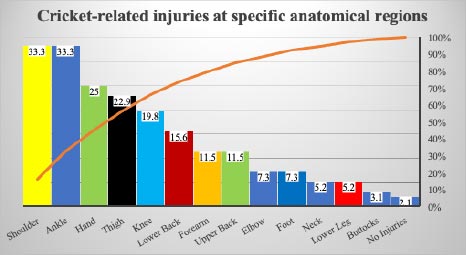
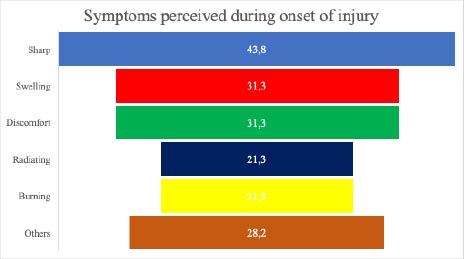
The anatomical sites of cricket-related injuries were: the shoulder (33.3%), ankle (33.3%), hand (25%), thigh (22.9%), and knee (19.8%) (Fig. 2). Results of symptoms illustrated in (Fig. 3) were sharp pain (43.8%), swelling (31.3%), discomfort (31.3%), radiating (21.9%) and burning pain (19.8%). Twenty-three percent of the symptoms lasted a few hours, 45.8% lasted a few days, and 27.1% were unpredictable. Similarly, 45.8% of the participants were out of the game for one week, while 34.4% were for only a few days. Injuries lasting longer than three months were rare (2.1%) and involved ruptured muscle fibres, torn ligaments, and bone fractures. The majority (85.4%) did not obtain healthcare. Increased pain or/and musculoskeletal pain after an injury was experienced by 61.5% when engaging in physical activity. Cross-tabulation of access to health care indicated that 64.6% of participants experienced musculoskeletal pain after physical activity with no healthcare service. This supports the previous result that participants (56.3%) reported playing through pain. Reasons for not seeking medical attention were: unnecessary (43.8%); used to play with pain (32.3%) and perception that the pain would go away (27.1%).
*Note: All values are percent of N = 96
*Note: All values are percent of N = 96
| Prevalence and type of Cricket Injuries | Body Limb | % | Av Injury | % | Types of Injury | % |
|---|---|---|---|---|---|---|
| Upper limb | 51.0 | Overuse | 45.8 | Strain | 41.7 | |
| Lower limb | 45.8 | Traumatic | 30.2 | Sprain | 49.0 | |
| Head & neck | 3.1 | Both | 24.0 | Bruising | 47.9 | |
| - | - | - | - | Fracture/laceration | 17.7 | |
| Mechanism of Injury | Context of Injury | % | Mechanism of Injury | % | ||
| Game match | 68.8 | Collision | 8.3 | |||
| Training session | 57.3 | Struck by ball | 41.7 | |||
| Other PA | 31.3 | Rapid rotation | 44.8 | |||
| Others | 3.1 | Overuse | 51 | |||
| Training History | N | Min | Max | Mean | SD |
|---|---|---|---|---|---|
| Months | 96 | 3 | 10 | 5.59 | 1.278 |
| Week (days) | 96 | 2 | 5 | 3.38 | 0.785 |
| Duration (hours) | 96 | 2 | 4 | 2.81 | 0.509 |
| Intensity (1-10 Borg Scale) | 96 | 5 | 10 | 6.81 | 1.136 |
The effects of injury were as follows: bowling speed reduced (49.4%); altered bowling action (34.4%); reduced number of overs bowled per game (33.3%); a restricted range of shots (42.7%) and changing technique (40.6%) for batting; and for fielding, throwing speed (39.6%) was reduced, throwing technique modified (36.5%) and others (44.8%). The common injuries/musculoskeletal pain that transpired within 5 yrs amongst the participants were: ankle sprains, bruising, lower back pain, open wounds, hamstring strain, shoulder injury (rotator cuff impingement), and concussions. The vast majority of the participants, 79 (82.3%), reported not having access to healthcare practitioners in their respective community clubs, while only 9 (9.4%) did have and the remainder responded ‘Maybe’ 8 (8.3%).
4. DISCUSSION
The average training time was 2.81 hours (168.6 min), 3.38 days per week, and 5.59 months a year. Overall average intensity of 6.81 (Borg scale 1-10) was exhausted per training session. Core stability and flexibility were the least acquired after training (1%). Almost half of the players (45.8%) participated in additional physical sports activities. Younger players were more likely to engage in additional sports compared to older players. The younger group (N = 44) was associated with additional sports other than cricket-related activity. By comparison, those who did not (N = 52) who did not participate in additional sports activities were associated with numerically older age groups. To test the null hypothesis, an independent T-test was performed. The assumption of homogeneity of variances was tested (equal variance not assumed) with Levene’s F test. The independent sample T-test was associated with a statistical significant effect.
The key findings of the study were that the majority (90.6%) of the participants reported having an injury or related musculoskeletal pain in a single season; the upper limb (51%) was prevalent, followed by the lower limb (45.8%). Prevalence in descending order of the anatomical sites was shoulder (33.3%), ankle (33.3%), hands (25%), thigh (22.9%), and knee (19.8%), which is to be expected as these are the predominant body parts used in cricket games in their order of usage. These findings support several international and local cricket injury studies in competitive cricketers [3, 4, 7, 9]. Most of the injuries are sustained by bowlers, followed by fielders [8]. Overuse (45.8%) injuries were prevalent compared to traumatic (30.2%) in the current study. An overuse injury is caused by a repetitive or chronic injury that lasts over a period, whereas a traumatic injury is a single incident that causes an acute injury [8]. Similarly, young players sustain more overuse injuries than senior players and are likely to be involved in additional physical sports [3, 7]. All-rounders (40.6%) were dominant in the study, and previous studies support this finding in community cricket and junior level [4, 5, 7, 10, 13]. Young players are likely to be involved in all aspects of the game, bowling, and batting, hence increasing their risk of overuse injury [7]. Gamage, Fortington, Kountouris and Finch [6] stated that strains and sprains are most common among junior cricket players: strains are tearing or damage to muscle tissue and sprains are tearing or damage to ligaments.
Shoulder was a frequent injury site due to repeated movements (shoulder extension, internal/external rotation, abduction, and elbow flexion/extension), which causes overstretch of the glenohumeral and acromioclavicular ligaments, biceps long head, and supraspinatus impingement at the subacromial space [12]. Some studies [9, 14] found that the surge in T20 cricket in recent years increased the overall workload per season among bowlers and the reduction in rest period has led to an excessive increase in injury prevalence. Hulin, Gabbett, Blanch, Chapman, Bailey and Orchard [11] & McNamara, Gabbett and Naughton [15] supported the findings, “Fast bowlers have greater match-play workload requirements and are at greater injury risk than other positions”. Fast bowlers and batmen had a high rate of hamstring strain related to running [5]. Bowlers also play a role in fielding. Studies based on onset injury found that bowlers were most likely to sustain acute traumatic injuries during fielding compared to bowling, indicating poor fielding techniques [3, 4, 7]. Bowling and batting account for most overuse injuries, with acute traumatic injuries being prevalent in fielding [4, 6, 7].
Majority of injuries occurred during game matches (68.8%) which supports previous studies of competitive and community cricket levels [4, 7]. About the mechanism of injury sustained overuse injuries and rotation movement (rapid twisting) were prevalent. Injuries in community cricket had a high prevalence of bruising and laceration (traumatic events resulting in open wounds), which was found to be the second most prevalent in this study. Ahearn, Bhatia and Griffin [16] and Russell, Hughes, Heskin and Lee [10] supported the finding that fielding players suffered more acute injuries during the game due to direct blows and contact with the ball. According to McLeod, O’Connor, Morgan, Kountouris, Finch and Fortington [7], community cricket players lack adequate skills in catching and throwing. Inadequate skills result in moderate to high rates of bruising relating to misfielding and being struck by the ball, contributing to the rate of traumatic injuries.
Regarding the symptoms associated with the injuries sustained, the most prevalent were sharp pain, swelling, discomfort, radiating pain, and burning sensation. Finch, White, Dennis, Twomey and Hayen [13] indicated in a community level study that sharp pain, bruising, and swelling due to being hit by the ball were common. Muscle pain is associated with sharp swelling, bruising, and discomfort pain sensations, but neurological pathologies are associated with pins and needles and radial pain sensations. Musculoskeletal pain was more prevalent than neurological pain [8]. Sharp pain, swelling, and discomfort resulted in the participants being out of play for a short period. There was a reduction in long-term injuries; the majority of long-term injuries are trauma-based; as previously stated, cricket is more of an overuse sport since it is non-contact [12, 13, 17]. This study concurs with the findings of Gamage, Fortington, Kountouris, and Finch [6] protective equipment in community level cricket is grossly lacking. It is now a requirement to wear protective equipment during batting and fielding (gloves, thigh pad, helmet, tapping fingers). However, Gamage, Fortington, Kountouris, and Finch [6] found that protective equipment was not compulsory at the community cricket level. Coaches and umpires must ensure protective equipment is always worn.
There is a difference between competitive and community level cricket based on the intensity and risk factors endured by players [17]. Several risk factors, especially extrinsic (environmental), affect mostly the bowling end of the game due to the various landing techniques players use while bowling, especially fast bowlers. The high-intensity short format twenty overs (T20) and fifty overs (One Day International) were prevalent in the study. Playing surface (rolled grass, soft concrete, artificial turf) was one of the contributing factors in the study. The type of pitch impacts injury prevalence; the absorbing force when landing differs between pitches, as results from the study indicate grass (53.1%) and concrete (41.7%) are implicated. Hard cricket pitches contribute to the lower back, knee, and ankle injuries with mechanisms including ankle supination/pronation, knee hyperextension, and knee varus/valgus force. Two studies conducted in Australia considered cricket pitch hardness as risk factor in lower limb injuries [9, 18].
Five months on average, was spent in training sessions among the participants, with three days per week most frequently. In a South African Schoolboy cricket study, less than 3.5 days of training is adequate for cricket as it can increase the rate of injury [8]. The lack of flexibility and core strength in the training sessions is alarming, knowing fully well that flexibility training helps an individual to become more resistant to pain or injury, overcome muscle stiffness, and give a greater range of motion. Safe strength (core stability) training at this point in a cricketer’s development enhances resilience in bone, tendons, ligaments, stability, and muscles, resulting in fewer injuries and improved performance. Therefore, more strength and flexibility training may be initiated to reduce the chances of injury and pain [8]. Due to several reasons, including occupation as a main factor, players differ in training schedule, alluding to inadequate physiological adaptation. The importance of rest physiologically is essential for regaining homeostasis, replenishing muscle glycogen, muscle recovery sustained from any damage, and overall maintenance of fitness. Several cricket coaches undermine the optimal importance of rest and muscle damage, which contributes to the overuse injury rate [3]. Among the participants, 45.8% (p = 0.209) were involved in other sporting codes, while the inferential T-tests indicated no statistically significant difference with age (junior and senior cricketers). However, Noorbhai, Essack, Thwala, Ellapen. and Van Heerden [8] reported that 62% of Schoolboy cricketers participated in addition to physical/sports activities during the off-season, indicating that young players may be involved in other sporting activities.
There is a lack of primary health services in community cricket [10]. Basic primary healthcare in community cricket, such as first aid, is essential in injury/musculoskeletal pain early treatment. It is a fact that most community cricket players lack a primary healthcare injury treatment apparatus, with 85.4% of participants in the study reported not obtaining medical treatment [7]. Untreated microtrauma overuse injuries in time lead to tendinopathy, microfracture, and ruptured muscles/tendons. This leads to contraction with an increase in pain and a further decrease in physical activity. The lack of healthcare in community cricket is not widely researched; it is necessary for the advocacy of injury prevention knowledge among community cricketers. Injury and musculoskeletal pain affect all aspects of the game (batting, bowling, and fielding). Reduced bowling speed, altered action, and reduced number of overs can, therefore, reduce the overall workload. Reductions in restricted shots and changing technique were highest in batting. Once injured by the ball, a player’s psychological view of the game changes. During this current time, mental health in sports is on the rise, according to McCabe, Peirce, Gorczynski, and Heron [19]; cricketers are at higher risk for stress, anxiety, depression, and adverse alcohol abuse. This calls for the advocacy of prevention of musculoskeletal pain, overuse injuries, and mental illness, with more research needed in community cricket. The prevalence of risk factors and injuries is not well investigated. Most prospective injury data in community cricket have been focused on junior-level and school cricket with little information on adult community cricketers.
The community management (coaches) should have a basic knowledge of physical fitness, player injury information, and the mechanisms common to preventing future injuries. Coaches also need to be educated on basic healthcare, including but not limited to First Aid.
5. LIMITATIONS
Reliability and validity are among the major limitations of studies on self-reporting of injuries. Due to the COVID-19 pandemic, a recent cricket season could not be analysed in a longitudinal study. As such, the mechanism, prevalence, risk factors, and anatomical sites of injury were recalled from the season before the pandemic. Due to potential contrasts in the degree of discernment and comprehension of the injury component among community cricketers (generally youngsters), the terms for various injury types (for example, stretch/damage tendon or muscle; damage or stretch ligament: sprain) were simplified. Several epidemiological studies report injuries based on the number of hours or playing days. For this study, injury per player was used and relied on player self-reporting recall (due to the pandemic). Injuries sustained were not validated by a healthcare practitioner and the onset of injury was not recorded. Ideally, it would have been useful to incorporate both measures. The possibility of collecting data was impractical. Players’ low-rate response was a further study limitation.
CONCLUSION
The study showed a high prevalence of overuse injuries among community-based cricket players. Upper limb injuries were most common, with overuse as the mechanism. The shoulder and ankle were the most injured anatomical sites, also due to overuse. The high prevalence of injuries sustained by players when struck by the ball occurred mostly during a match. Inadequate training, pitch hardness, and knowledge of injury prevalence were highly rated as risk factors contributing to an increase in injuries. The study highlighted the lack of primary healthcare at the community cricket level. Further South African longitudinal studies are required at the community club level with a larger population variety across community settings.
AUTHORS' CONTRIBUTIONS
HN conceptualised the paper. SZ collected the data. YA conducted data analysis. All authors contributed to the write-up and revision of the paper before submission.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical approval was sought from the Faculty of Health Science Research Ethics Committee (REC-775-2020) at the University of Johannesburg, South Africa.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Informed consent was obtained from all the participants and data collected during the study were kept strictly confidential.
STANDARDS OF REPORTING
STROBE guidelines were followed.
AVAILABILITY OF DATA AND MATERIALS
The data and supportive information are available within the article. Due to the privacy and anonymity of the participants' data, the data is available from the corresponding author [H.N] upon reasonable request.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

