All published articles of this journal are available on ScienceDirect.

Determinative Factors in The Injury Incidence on Runners: Synthesis of Evidence “Injuries on Runners”
Authors Info & Affiliations
Abstract
Background:
Long-distance running is a popular recreational exercise. It is a beneficial activity for health and wellness. However, the running can also cause injury, particularly in the lower extremities. There is no consensus in the literature on the intrinsic and extrinsic factors that cause these musculoskeletal injuries. In theory, most injuries are caused by methodological errors, the type of footwear and terrain.
Objective:
To identify the factors associated with injuries in recreational runners based on evidence.
Method:
The data sources used were: PubMed, Science Direct and Web of Science. Compiled the English-language articles identified by keywords, titles of medical affairs and research of electronic databases above. With this research from the review process, controlled trials were grouped in a study population consisted of recreational runners.
Results:
Evidences suggest that injuries are common for runners. Many variables can contribute to the injury process, among them extrinsic factors such as training methodology, running shoes and surface.
Conclusion:
To modify one or more of these factors may help prevent injury, so coaches and runners should consider it, and prevention efforts need to be tailored to this group to reduce the risk of specific injuries.
1. INTRODUCTION
In the mid-1970s there was an intense adherence of society to exercise programs in response to the divulgation of the related benefits. Until the 1980s, about 25 million people have begun to run only in the United States [1]. The running is currently one of the physical exercises that has acquired great popularity around the world [2]. The benefits attributed to the regular practice include improvements in physical and mental health, weight control, stress reduction and socialization [3, 4]. After a while running regularly practitioners report changes in lifestyle, including better eating habits, improving sleep quality and reducing alcohol and tobacco intake, feel happier, relaxed and energized [2]. However, the potential for injuries related to running has been evidenced over the past decades by various researchers.
In the 1980s the incidence of injuries in runners was 60% [5], in 1990 about 70% [6], currently the researchers estimate that about 92% of the regular runners may acquire some type of injury during some time of the year [7]. The broad spectrum of these epidemiological findings can be attributed in part to differences in definitions of “Runner” and “Injury” [8]. The literature has typically featured a “Runner” who runs a minimum distance of 3 km per session [9], regularly (three times a week) [6], and been consistent in the minimum of one year [6, 9]. The definition of “Injury” also varies between studies; however, a common definition assigned to running injuries is the musculoskeletal one, characterized by a running speed restriction, distance, duration or frequency for a minimum period of one week [10-12].
Exposure to the risk of injury related to the movement required in sport [2]. Microleaf and regeneration represent a normal process associated with training. However, exacerbated exposure coupled with multifactorial aspects may culminate in overuse injury [13].
Several researchers have speculated the nature of the injuries in runners. According [14], 60% of running injuries have been attributed to training errors, however, studies indicate that injuries result from a combination of intrinsic factors such as; biomechanical abnormalities [15], sex and body mass index (BMI) [16], postural deviations [14]; anthropometry [12]; previous injury [1]; technical experience [6, 17]; mobility of the foot sole [10]; high longitudinal arches (pes cavus) [18]; muscle weakness, genu varum knee, hip high in Anglo Q [19]; poor flexibility [20]; as well as extrinsic factors, such as methodological misunderstandings, namely the intensity, volume, frequency of running [20-25]; unsuitable footwear, and surface [26, 27]. Identifying the factors associated with injuries is the first step in the process of prevention. However, there is no consensus in the literature on the intrinsic and extrinsic factors that cause these injuries, hence, the purpose of this study was to identify the factors associated with injuries in recreational runners based on evidence.
2. METHODOLOGY
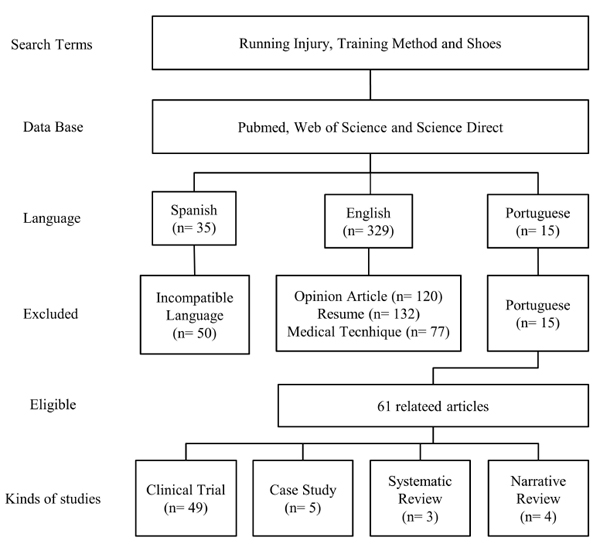
In this review we consulted the electronic databases: Pubmed, Web of Science and Science Direct retrospectively without date restriction, Science Direct retrospectively without date restriction, using the keywords: Running Injury, Training Method, Shoe and Surface. The search was in English between the 2nd and the 16th of September, 2015. The search was in English. Articles identified by the initial search strategy were evaluated independently by two authors, according to the following inclusion criteria: 1- population (recreational runners), 2- intervention (musculoskeletal injuries). Articles in another language or that had repeated information or available in other articles were excluded. Such inclusion and exclusion criteria were applied when there was disagreement of opinion between the assessors. Previously, it was selected 379 works by the title of the content. After reading the abstracts, 317 were excluded for not meeting the inclusion criteria: 50 because they were in other languages, 109 because they were opinion articles, 59 because they were about medical techniques and 99 for having only the summary available for review. Thus, 62 studies were included for the stage of critical analysis (Fig. 1).
3. INCIDENCE OF INJURIES
The purpose of this study was to identify the factors associated with injuries in recreational runners based on evidence. An analysis of 2,000 runners revealed that about 42% of injuries occurred at the knee [9], followed by plantar fasciitis and tibia stress syndrome. The authors also found that the higher prevalence of lesions focused on physically active people with less common practice than eight and a half years. In addition, women with a body mass index less than 21 kg/m2 are positively associated with a significantly increased risk of fractures due to tibia stress and spinal injuries. Kluitenberg [28] it was evaluated 1,696 recreational runners who underwent a 6-week program, who described in a daily journal complaints relating to injuries in the running. There were no significant differences between the anatomical locations and injuries that were recorded. The main causes of removal were located in the knee, hip, sacrum iliac region and buttocks. The incidences of injuries were related to the impact generated by the successive shocks of the feet on the ground. Other studies have also determined that the knee injuries represent approximately half of all injuries related to running [5, 13, 22]. The foot, ankle and leg comprise almost 40% of the remaining lesions, whereas less than 20% occurred over the knee.
Runners are particularly affected by chondropathy patella, patellar tendinopathy, the tibia periostitis, the ilio-tibial tract friction syndrome, plantar fasciitis and calcaneal tendinopathy. This suggests the possibility of the existence of a common mechanism in the etiology of injuries in the running [29]. The runners suffer from acute injuries such as sprains and ankle fractures, but the majority of running injuries may be classified as overuse, or injury from overuse [9]. An overuse injury has been defined as a musculoskeletal injury resulting from the combined effect of fatigue over a period of time beyond the specific structural capacity [1, 13]. Quantitatively injury rates increase significantly when the weekly mileage exceeds 40 miles cumulatively [19]. Although the repeated stresses on various musculoskeletal system structures result in a stress injury, this does not mean that the stress should be avoided [29].
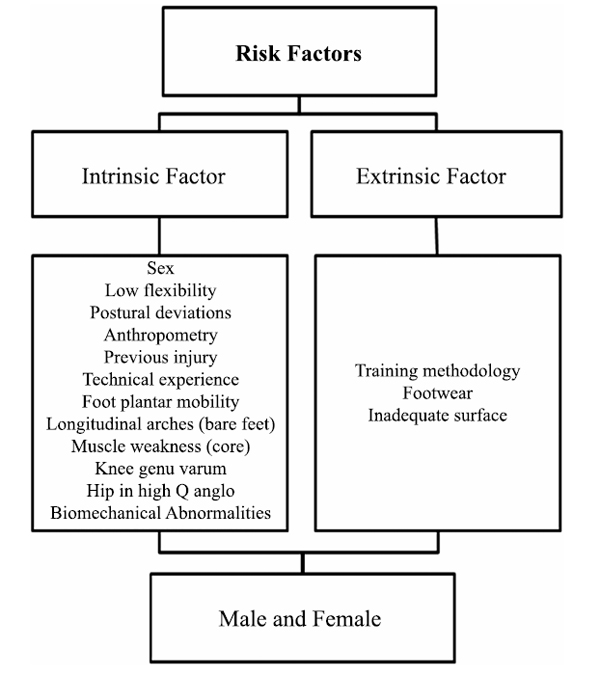
The biological structures, such as muscles, tendons, ligaments and bones, can adapt to the positive or negative voltage level that is imposed on them [30]. This phenomena leads to positive remodeling, as soon as there is an adequate period of time between stimuli, whereas any acute stress is insufficient to generate adaptations and trigger lesions [6, 30]. Runners that developed passed standards that incorporate relatively low levels of impact forces, may vary in magnitude from about 1.5 to 5 times the body weight and a low rate of pronation are less susceptible to injury from overuse [31, 32]. The literature discusses how risk factors are conceptualized in the investigation of sports injuries; these may be intrinsic or extrinsic (Fig. 2).
The injuries result from the complex interplay of factors. Table (1) shows the environmental risk factors modifiable and non-modifiable categorized by the consensus of experts.
| Modifiable Risk Factors | Non-Modifiable Risk Factors |
|---|---|
| Adversary [20] | Sex [16] |
| Altimetry [33] | Knee genu varum [19] |
| Anthropometry [16] | Hip in anglo high [19] |
| Technical experience [17] | Previous injury [1] |
| Flexibility [20] | Biomechanical abnormalities [15] |
| Surface [4] | Rules [9] |
| Shoe [2] | Unforeseen events [34] |
| Training [35] | Postural deviations [36] |
| Meteorological conditions [37] | |
| Muscle weakness [19] |
It is important to note that certain risk factors classified as non-modifiable may be altered by surgical interventions (e.g., the angle of tibia slope) or pharmacological (e.g., menstrual cycle and hormonal concentrations), but such measures are not viable or ethical. On the other hand the modifiable risk factors categorized as, e.g., weather, rules surface and may not be financially feasible or social to change, which would affect the successful implementation of injury prevention programs. Currently the researchers focus on the risk factors for modifiable injury in runners, these include anatomical variations between runners [38], neuromuscular control [39], factors Biomechanical that affect how to run the motion, muscle strength [35], fatigue during the landing of the foot on the ground [3], the running shoes [40] methodological mistakes, heating, stretching, errors nutritional and psychological factors [20].
3.1. Training Methodology
Running is a popular activity and can be practiced everywhere [16]. Many runners complete a few kilometers just for fun, some of them do not participate in competitions. These recreational runners are probably the most common group in community halls. Among the factors highlighted by experts as the injury risk factors in corridors there is the training methodology. The identification of the training-related errors represent a line of interest particularly important knowledge, mainly in the prevention of running injuries [41], where the volume and weekly frequency are necessarily risk factors for developing lesions [35].
Moreover, the training system of corridors is easily changed, thus, understanding this synergy becomes a prerequisite to efficiently prevent injuries in this population. van Gent et al. [4] presents the main risk factors significantly related to injury in the running as excessive weekly distance, previous injury, lack of racing experience and participating in competitions. The author states that all overuse injuries are the result of training errors. From this point of view the lesions are caused by a disturbance of the external load applied to the biological body and this threshold structure. In this dose-response relationship [3], argue that there are four components applicable to the hallway. The first component is the current status of the musculoskeltal system. The second is the type of stress applied. The third factor, the frequency, intensity and duration of applied stress and finally the time of adaptation and recovery between running sessions.
Junior et al. [42] conducted a prospective cohort study with 200 recreational runners followed for 12 weeks. The runners answered an online survey on the bi-weekly workout routine, it was evaluated running experience, weekly frequency, distance and duration of the session, flooring type and terrain, type of training, level of motivation and participation in tests. The incidence of lesions in these corridors was 31% for every 1,000 hours of exposure. The most frequent type of injury was muscular injury and the most affected anatomical region was the knee. The relevant risk factors for the incidence of musculoskeletal injuries were the speed training, while the protective factor identified was the interval training.
Under normal circumstances, the musculoskeletal system adapts to the level of the applied stress [31]. When an optimal level of stress is applied to the musculoskeletal system, along with an adequate recovery time, the musculoskeletal system becomes stronger. On the other hand, when the applied voltage is too high or the recovery time is very short the fabric of the musculoskeletal system weakens, and the probability of suffering a subsequent stress injury increases [43].
The mechanical load applied to the human body can cause a physiological or pathological adaptation resulting in training effect, respectively, to the overuse or injury [44]. The musculoskeletal system of the recreational runner is usually not adapted to the repetitive impact forces and relatively high execution, especially beginners, are physically inactive, suffering a high biomechanical load from the start of the program in terms of frequency, intensity and duration [16].
Such as running involves several eccentric contractions, it seems that the eccentric strength training is plausible and could be beneficial to help runners to avoid injury [3]. Although there is no evidence of the benefit of eccentric strengthening in the treatment of patellar tendinopathy, Achilles tendinopathy, SPF, and hamstrings contractures, there is no primary prevention studies in corridors. A systematic review of eccentric exercises for Achilles tendinopathy showed promising results [45]. Because Achilles tendinopathy and SPF are common injuries in runners, a further study is warranted in eccentric exercises for primary prevention of these injuries. One of the most common mistakes that leads to injury in runners is the excessive mileage [4, 20, 31].
van Gent et al. [4] estimated that 60% of injuries were caused by methodological mistakes in practice, half attributed to excessive mileage. Other studies suggest that sudden changes in mileage [121] and the increase in this weekly mileage greater than 64 kilometers in men were associated with an increase of 72% in the risk of injury [4, 20] as well as in runners who train all year [46]. Another studied risk factor is experience; however, the results are conflicting. In elite marathon runners, hamstring and knee injuries were more common, but experienced runners had more injuries related to the foot [4]. Macera et al. [47] showed that runners with less than 3 years’ experience had high risk of acquiring injury.
Another study with cross-country runners showed no significant difference in injury rates between those with up to 3 years of experience [33]. The sudden increase in distance or weekly mileage change in workout type (in the hills) and accented interval work has been shown to increase injury rates. These aspects were highlighted in studies of military recruits. Those who initiated gradually through a basic training obtained fewer lesions [48]. Although [20] have found a direct correlation with increased speed and lesions, most studies show no association between the training speed and the risk of injury [4.11,33].
Each mesocycle is followed by a recovery period of approximately one week for the physiological adaptations before starting the next mesocycle. The subsequent incremental mesocycle adds greater intensity, duration or volume than the previous mesocycle. There are a large number of variables that compose the training using methods with different intensities, durations of stimuli and recovery intervals. However, the ideal methodology is far from being determined. Thus, it is recommended that training routines be checked and methodological misunderstandings identified so that the training program addresses individual adaptive responses.
3.2. Running Shoes
In the 1970s, the cushioned running shoes revolutionized the sports, at the same time, this long-distance running has gone from an elite competition to a regular exercise for the masses. Sports physicians discuss the importance of quality footwear (damping vs motion control), in a view of preventing and treating injuries. Traditionally the design is that using a quality shoe with cushioning will reduce the risk of injury [23, 49].
To the usual runners, the factors that influence the acquisition of running injuries are; run with inappropriate shoes for foot type; with inappropriate footwear for the type of steeping; and footwear without damping [3]. In addition, they express concerns about the lack of cushioning, heel height, excessive wear or footwear usage time [2]. Musculoskeletal injuries can be encouraged by the running shoes [26, 27, 50-52], these empirical evidence injuries aggregated with the overuse [29], result for logical reasons, however, until now, the association between footwear and incidence of injuries in runners are just hypotheses.
An intervention that is affordable for most runners is the selection of running shoes, however, for some people the options available in the market may create some difficulty in choosing. Essentially, because it is inferred that the ideal footwear minimizes the impact forces and provides stability and allows the foot a natural pronation [53], and these aspects indicate a reduced risk of injuries in the running [31].
This hypothesis is refuted and considered by Nielsen et al. [38] a myth of sport science. The researchers conducted a prospective cohort study recruiting 927 runners with an average age of 37 years of both genders who underwent running of 10 km and did not participate in other sports for longer than 4 hours per week. Each participant received a pair of neutral shoes (Adidas Supernova Glide 3), a GPS clock and access to a daily online training. Runners inserted 52 sessions in one year period and reported all the problems caused in this period that prevented them from carrying out the running for more than a week. They were examined by physiotherapists and sports doctors, and there was no difference in the relationship between the starting time of the first lesion and the Foot Posture Index in the 252 injured runners, moreover, the pronator had lower injury rate than runners with neutral feet.
A parameter considered essential in running shoes is its effect on the cushioning, stability and density (hardness) of the midsole. Although impact tests show that the footwear with softer midsole attenuate forces when compared to the harder footwear, there have been conflicting reports on the effects of varying the density of the midsole parameters of cushioning and stability [50, 51]. Recent studies have found that the softer shoes allow greater pronation rates than more rigid footwear [54], while others reported the opposite [52].
As lex Stacoff and Denoth [52] the footwear industry significantly changed the running shoes that we know in two main directions; the sole has become softer, which generally attenuate the shock during landing and reduced phase stability and, as a consequence; several features were made for the shoes increase the stability, in other words, control the pronation during the stance phase. In the databases with the terms “running shoes and injury” and “running shoes and prevention” there are many studies on the function of running shoes from the kinematic point of view, but we did not find studies that observe the prevention of clinical injuries, or post-exercise recovery. One reason for this gap is finding a good control group. Table (2) shows the differences between running with traditional and minimalist footwear.
A concept increasingly popular in the media (and literature) is running barefoot [57], where there is a reduction in the amplitude of the stepping and less impact from the midfoot to the forefoot, in opposition to the impact of the heel in cushioned shoes, it has been speculated that this attitude would reduce the risk of injury. In contrast, running on hard surfaces increase the risk of stress fracture and associated lesions. All articles about barefoot running so far are based on anthropological theory, it will be interesting to observe what causes injury and prevention in future studies.
In an attempt to analyze the available data objectively, Hreljac [29] conducted a meta-analysis of the existing literature. They determined that the shoes with more rigid midsole reduced the initial impact forces while greater mobility enabled during the initial stage of contact on the ground. They also noted that there was a lot of variability between individuals and between studies, indicating that individuals respond exclusively to the midsole stiffness changes. Thus, the footwear selection would require the corridor to carry out biomechanical tests in various running shoes to determine which one would best mitigated the impact forces and pronation rate, which is not a viable alternative. It would be preferable for the selection of running shoes for any individual to be based on two basic guidelines, be comfortable [58] and enable greater control [55].
The running shoes that meet these criteria provide optimal levels of damping and stability [59], which justifies speculation that the comfort is related to muscle activation, and therefore to the fatigue and the performance [29]. However, the few studies that have investigated the influence of running shoes in injuries in runners are different.
Nielsen et al. [38] conducted a prospective cohort study lasting a year, and found no significant differences depending on the distance before the occurrence of the first lesion between different types of stepped (highly supine, supine, prone, and highly prone) compared with neutral novice riders feet using the same type of footwear. Knapik et al. [60] conducted an analysis of the risk of injury among individuals with different shoes. One group received shoes with motion control, stability or neutral based on their foot type. Compared with those who received a shoe with independent stability of your foot type, there were no differences in injury risk between individuals.
Ryan et al. [61] observed that pronators runners using a shoe with movement control had a greater risk of injury than pronators using neutral footwear. The ideal running footwear must respect the physical, anatomical, physiological and kinematics of the corridors, in addition to producing satisfactory effect on the subjective feeling of comfort [28]. Aware of these requirements, the running shoe market offer products that promise to reduce the appearance of injuries and to prevent them.
| Traditional | Minimalist | |
|---|---|---|
| Foot contact [55] | Forefoot | Heel or half foot |
| Effect of footwear [26] | Not applicable | Provide cushioning / shock absorption. Mobility control. It affects the kinematics of the lower extremity (pronation / supination in the foot and ankle, internal rotation of the tibia / external) |
| Kinematic [28] | Increase of the moment of plantar flexion in the soil. Maximum knee flexion, 105°-130°. Frequency and amplitude of the upper pass | Higher level of dorsiflexion. Maximum knee flexion 90° |
| Kinetics [39] | Lower impact force on foot contact. Greater activation of the anterior tibial and gastrocnemius-soleus throughout the cycle | Greater impact on foot contact. Minor muscle activity of the leg versus minimalist, also dependent on the type of footwear |
| Economy [56] | Improved economy (under discussion) | Economy based heavily on training. Some suggest decrease versus minimalist condition |
| Injury Rates [40] | Unknown when compared with minimalist | Unknown when compared with traditional |
Clifton et al. [62], referring to the opinion of 585 runners as the importance of the performance attributes considered essential in running shoes, found that women give priority when acquiring to: i) consistency of damping; ii) traction; iii) durability of the sole; iv) absorption of impact; and v) weight of the shoe. The male sample prioritizes in the acquisition of running shoes: i) impact absorption; ii) stability; iii) durability of the sole; iv) the consistency buffer; and v) weight of the shoe. Two investigations in sports medicine have shown the need for guidance to the current practice.
One study evaluated more than 3,000 soldiers in military basic training. There was no difference in injury rates between the experimental group equipped for motion control, stability, or type cushioning of running shoes classified by the arc type (low, medium or high) vs the control group [40]. Richards et al. [56], in a review study in Medline, Cinahl, Embase, PsychInfo, Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled trials, Sports Discus and Amed, found that the choice of footwear running is not based on scientific evidence. In Pubmed in review with “running shoes and injury” and “running shoes and prevention” there are many studies on the role of running shoes from the cinematic point of view, we have not found studies that observe the prevention of clinical lesions, or recovery post-exercise. One reason for this gap lies in finding a good control group.
3.3. Running Surface
There are reports that running up and down slopes produce injuries, but no evidence has been found between injuries and surface. However, running frequently in slope can cause problems in the knee joints [27], because the weight of the body falls mainly on the vertical axis of this region, requiring that the quadriceps muscles work too hard to protect it. In the running downhill to an increase of knee flexion, extensor apparatus, patellofemoral forces and absorption of impact and contraction of knee extensors. Excessive running on the slope can cause damage to the calcaneal tendon and plantar fasciitis.
Running on the slope can create a functional leg length discrepancy. Functional shortening of the leg may also be a result of dysfunction of the sacroiliac joint, excessive unilateral pronation, lumbar muscle pain, contractures, or muscle imbalance. The leg length discrepancy may be associated with injuries such as iliotibial tract syndrome, trochanteric bursitis, lower spine pain, and stress fractures. In this sense, Van Gent, Siem [4] suggests that runners who make abrupt changes in duration, volume greater than 64 kilometers per week or work on uneven surfaces as trails, are more susceptible to stress fractures. Among the affected regions are tibia (25-59%), metatarsals (10-24,6%) and fibula (7-22,9%).
Some surfaces may triple or quadruple the frequency of lesions [26]. Running on hard surfaces, such as asphalt or concrete, causes mechanical shock and thus overloads joints and tendons, which may be associated with a higher incidence. Running on a very soft surface allows hypermobility of the joints, causes muscle fatigue and can result in overuse. Grass and earth are great surfaces for running, but on uneven, artificial surfaces or on slippery slopes can cause injury. Running on uneven surfaces or slopes to one side can cause abnormal tension on one side of the body, resulting in a functional leg length discrepancy that can cause medial tibial stress syndrome or trochanteric bursitis.
New studies randomized, controlled, need to be conducted to carefully define interactions between risk factors and the isolated effect of preventive measures.
CONCLUSION
Evidences suggest that injuries to runners are common. Many variables potentially contribute to the injury, among them extrinsic factors training such as methodology, running shoes and surface. To Modify one or more of these factors may help prevent injury, so the injury threshold should be considered by coaches and runners, and prevention efforts need to be tailored to this group to reduce the risk of specific injuries.
CONSENT FOR PUBLICATION
Not applicable.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

