All published articles of this journal are available on ScienceDirect.

Lower Extremity Injuries in Young Floorball Players: A Prospective Study on Overuse Injuries
Abstract
Background:
Overuse injuries in sports seem to be 1.5 to 2.5 times more common than traumatic injuries in the lower extremity (LE) in children and adolescents. Floorball is the most popular indoor sport in Sweden and is associated with many potential risks of injuries. However, to our knowledge, no previous studies have examined the appearance of injury in young floorball players.
Objective:
The aim of the present study was to investigate the occurrence of overuse injuries in LE in floorball players aged 15 or younger, with respect to frequency, location, and consequence of injury.
Method:
Fifty-seven players, from 9 different teams, participated (mean age 11±2 years). A modified version of Oslo Sports Trauma Research Center Overuse Injury Questionnaire was submitted every fourth week during five months in order to record overuse injuries in LE. An online survey software was used to send out the questionnaires.
Results:
A of 42 overuse injuries in 42% (24/57) of the cohort were found. The average monthly prevalence for all players, in any anatomical area, was 28% (95% confidence total interval 18%-38%). The most common location of injuries was the knee (43%), followed by the foot (40%).
Conclusion:
The present study shows, in accordance with other recent studies on children and adolescents that overuse injuries seem to be a common problem for young floorball players. Knee and foot appear to be the most common location for overuse injuries in this population. Prospective analyses of different mechanisms for overuse injury in youth athletes and the relation to growth-related overuse disorders is desirable.
INTRODUCTION
Floorball is a relatively new team sport that has become very popular during the last decade and is today the most popular indoor sport in Sweden [1]. However, floorball is associated with many potential risks of injuries, such as sud-den accelerations, stops and turns, hits by ball or sticks, and accidental body contacts with an opponent or the board [2, 3]. In Sweden, approximately 7200 players every year sustain floorball-related injuries that require emergency care [4]. Furthermore, almost 40% of these players are 20 years old or younger. The proportion of overuse injuries associated with floorball varies from 17 to 30% [2, 3, 5, 6] and the knee is the most common location for overuse injuries [2, 5]. Although previous studies have investigated the occurrence of injury in floorball [2, 3, 6, 7], all of them focused on adult players.
In general, the most common location of sport injury in children and adolescents is the lower extremity (LE) [8-10]. It has been noted that half of the injuries in children and adolescents are due to overuse [9-11]. Suzue et al. [12] reported that among 1162 junior soccer players, 44.1% complained of leg pain. Overuse injuries seem to be 1.5 to 2.5 times more common than traumatic injuries in the LE in children and adolescents [8, 10]. However, little information exists regarding floorball-related injuries in children and adolescents. It is our belief that future research is required to investigate the injury panorama in youth floorball and also to investigate the extent of the problem. Understanding injury mechanisms might lead to better development of preventative protocols, resulting in higher sport participation throughout life. Therefore, the aim of the present study was to investigate the injury panorama of overuse injuries in LE in children and adolescents who regularly participate in floorball. The intention was to provide insights on injury prevalence, injury location, and injury consequences.
MATERIAL AND METHODS
Subjects
A systematic sampling was carried out by a selection of 46 floorball teams from a register, compiled by the authors, of active teams with players born in 1999 or later in the region of Halland, Sweden. Team coaches of the selected teams were contacted and provided with written information. The coaches then provided written information to each player’s parents. The parents were asked to complete data in a pre-printed form regarding the player’s team affiliation, sex, date of birth, weight, height and number of hours per week the player participates in organized floorball training and matches, and in other organized sports activities besides floorball. The parents were also asked to provide a current e-mail address and submit this, along with a signed consent form, to the coach. Each coach collected all consent forms and submitted them to the author. A separate information letter was also sent to the players with simplified information about the study. If the parents considered that their child (player) themselves could take a decision concerning their participation in the study, the player was asked to sign the consent form and send it to the author, either digitally or by ordinary mail. Ethical approval was obtained from the Southeast Ethics Committee.
Experimental Design
Data was collected every four weeks over five months, from 24 November 2013 to the end of the season in March 2014. The last questionnaire was collected on 30 March 2014. The questionnaire was sent out to each player by an online survey software, WebbEnkäter, enuvo GmbH, Zürich German, to the e-mail address provided by the player. The injuries were self-reported by the players and all physical complaints were defined using the descriptions by Clarsen et al. [13]. A reminder email was sent out if no response was received within three days, and a second reminder was sent after seven days without a response. The survey software prevented submission of incomplete questionnaires, and the questionnaires could not be completed more than once per event and person. In the context of the third questionnaire dispatch, a new separate information letter to the player was sent out, asking to complement the consent with the permission for remaining participation in the study.
Measurements
The Oslo Sports Trauma Research Center (OSTRC) Overuse Injury Questionnaire [13] was used to record the occurrence of overuse injuries in the LE, pain levels and the consequences of injury on sports participation and sporting performance. The OSTRC Overuse Injury Questionnaire is a valid instrument and has been tested for high internal consistency, Cronbach’s alpha (α) 0.91 [13]. The questionnaire was translated from English into Swedish and modified for this study by the authors. The questionnaire included questions on the consequences of overuse problems at the hip, knee, lower leg, and foot. A short summary was presented, before each question area, explaining that all questions should be completed regardless of whether the athlete had experienced any problems in that area. In the summary, examples of the most common overuse symptoms for each area were also given. In order to differentiate acute injuries from overuse injuries, the question “How did the physical complaints, specified above, occur?” was added to each part of the questionnaire. In this study, an overuse injury was defined as “any physical complaint sustained by a player, irrespective of the need for medical attention or time loss from floorball activities,” based on recent recommendations on definitions of overuse injuries [14]. Hence, all complaints that did not have a sudden traumatic onset were regarded as overuse injuries.
In order to obtain views about the design, to achieve face validity of the translated and modified questionnaire, and to determine the internal consistency, the questionnaire was preliminary tested on a group consisting of 13 parents who had children playing floorball. To determine test-retest reliability a retest was carried out after one week. In order not to influence the results, the parents were not informed about the purpose of the pilot study until the second dispatch.
Statistical Analyses
For each four-week period, the injury prevalence for each anatomical area was calculated by dividing the number of individuals who reported any problems in this area by the number of questionnaire respondents for the same period. Similar calculations were carried out for the number of reported problems that led to moderate or severe reduction of training volume or moderate or severe reduction in athletic performance or complete inability to participate in sport, corresponding to the options of responses 3, 4, or 5 in either question 2 or question 3. This corresponded to the prevalence of substantial overuse injuries. The mean for these above mentioned calculations was calculated for each anatomical area; the average monthly prevalence of all problems and the average monthly prevalence of substantial problems were also calculated. A 95% confidence interval (CI) was calculated for all variables.
Statistical Package for the Social Sciences (SPSS) software version 22.0 was used for the statistical calculations. The Cronbach’s alpha (α) was calculated to examine the inter-item correlation in the scale. To examine test-retest reliability, that is the degree to which patients can be distinguished from each other [15], two-way random intra-class correlation coefficient for absolute agreement (ICC2, 1) was calculated [16]. The measurement error, i.e. exactly how close the scores for the repeated measurements were [17], was presented by the standard error of measurement (SEM). The level of significance was set at p<0.05.
RESULTS
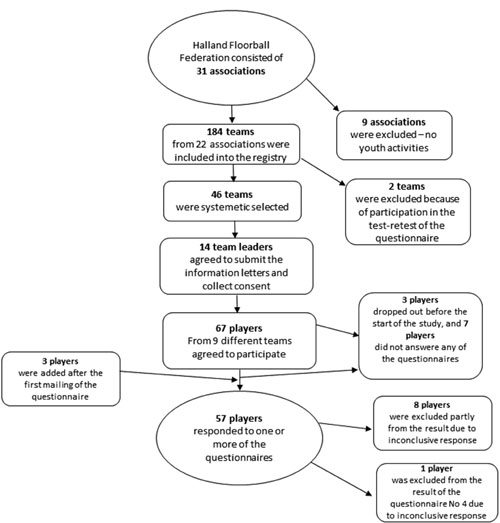
Fourteen coaches, from a total of 46 selected teams, agreed to submit information letters and collect the consent forms. Sixty-four, out of 179, players from nine different teams agreed to participate in the study. Finally, a total of 89% of these (57/64) participated on one or more occasions during the course of the study. The average response rate for the questionnaire was 78%, with 56% (32/57) of the participants responding to all of the five questionnaires. Further information on the sample and study process is presented in detail in Fig. (1). Table 1 shows descriptive statistics for the full sample.
| Total | Girls (n=15) | Boys (n=42) | |
|---|---|---|---|
| Age (year) | 11 (2)a | 10 (1)a | 12 (2)a |
| Height (cm) | 151 (15)a | 142 (8)a | 154 (15)a |
| Weight (kg) | 42 (13)a | 33 (7)a | 46 (13)a |
| Training hours / week | 3.57 (1) a | 2.97 (1) a | 3.79 (1) a |
Injury Frequency and Prevalence
A total of 75 overuse conditions were registered in 220 completed questionnaires during the study. Over the entire period, and when repeated reports of a complaint in the same anatomical area were regarded as a single overuse injury, a total of 42 overuse injuries in 42% (24/57) of the cohort were found. When repeated reports of a complaint in the same anatomical area, despite intermediate reported periods of non-complaints in the particular anatomical area, were regarded as a single overuse injury, a total of 33 injuries were registered. Further, if participants that only participated once or twice were excluded, a total of 39 overuse injuries were identified in 47% (22/47) of this group. The average monthly injury prevalence for all players, in any anatomical area, was 28% (95% confidence interval (CI) 18%-38%) and 6% (95% CI 3%-9%) for all substantial conditions (Table 2).
| Hip/pelvis | Knee | Lower leg | Foot | |
|---|---|---|---|---|
| Prevalence (all problems) | ||||
| Questionnaire 1* | 6 (3/50)a, b | 13 (7/52)a | - (0/52)a | 21 (11/52)a |
| Questionnaire 2* | - (0/50)a | 12 (6/49)a, c | - (0/50)a | 12 (6/50)a |
| Questionnaire 3^ | 2 (1/46)a | 17 (8/46)a | 2 (1/46)a | 22 (10/46)a |
| Questionnaire 4* | 5 (2/38)a | 16 (6/37)a, c | - (0/38)a | 11 (4/38)a |
| Questionnaire 5^ | 3 (1/36)a | 17 (6/36)a | - (0/35)a, c | 8 (3/36)a |
| Average | 3 (0.3-6)d | 15 (12-18)d | 0.4 (-0.8-2)d | 15 (7-23)d |
| Average prevalence (substantial problems) | - | 2 (0.5-4)d | - | 4 (3-6)d |
Injury Location
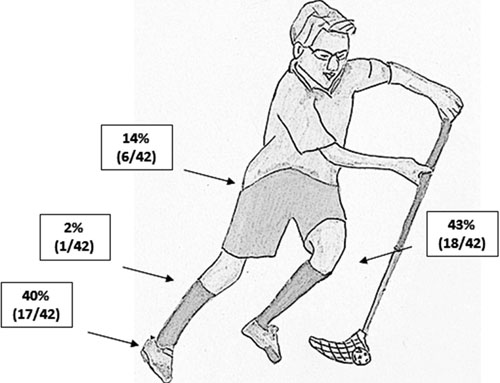
Twenty-five percent (14/57) of the cohort reported overuse conditions affecting the knee, and an equal number of players were affected by conditions in the foot. Nine percent (5/57) of the cohort suffered from a substantial problem at some stage during the course of the study. The distribution of the total number of registered injuries is shown in Fig. (2). Of all registered overuse conditions, 19% (14/75) were classified as substantial overuse injuries where the foot was the most affected body part, at 64% (9/14). Thirty-six percent (5/14) were registered in the knee.
Consequences of Injury
Of the injured players, 88% (21/24) reported, on at least one occasion, that they fully participated in training and competition but with problems. Seventeen percent (4/24) reported that the injury, on at least one occasion, led to reduced participation. Only one injured player reported a problem that involved minor pain that had no consequences for participation in sports activities. All registered overuse conditions resulted in at least minor pain on one or more occasions during the study. Of the injured players, 33% (8/24) had at least one injury that led to moderate pain, and all these injuries were located in the knee or the foot.
Pilot Test of the Questionnaire
The Cronbach’s α statistic was 0.891. Eleven parents participated in the retest of the questionnaire, and their result was used in order to calculate ICC and SEM. The mean score of the questionnaire was 1.09 (±0.18) on the first occasion and 1.13 (±0.18) on the second occasion (n=11). The ICC 2,1 was 0.876 and SEM was 0.06.
DISCUSSION
The main finding in the present study was that a total of 42 overuse injuries were found in 42% of the cohort. Further, an average monthly injury prevalence of 28% was found in the LE. This injury prevalence might be considered high but is in line with the results of Suzue et al. [12], who reported a point-prevalence of overuse injuries, confirmed by a medical examination, of 33% in junior soccer players in Japan. Clarsen et al. [5], who also used the OSTRC Overuse Injury Questionnaire for injury registration, found that the average prevalence of all overuse injuries in the knee, lower back, and shoulder were 27, 29, and 15% respectively in elite floorball players with a mean age of 22 years. In the present study, the average prevalence of reported knee problems was 15%. However, comparisons of the results are limited since age is a risk factor of injuries [11, 18]. Among other athletes, prevalence of overuse injuries of 31% in handball and 23% in track and field athletes have been reported [19, 20]. The participants in these studies were all elite athletes aged 15 years or older, hence a higher prevalence of overuse injuries is expected. Retrospective studies, such as the study conducted by Jacobsson et al. [19], are also expected to yield a lower injury rate than a prospective study. This also applies to the choice of definition of injury, where a “physical complaint” definition is expected to capture a higher number of overuse injuries than other, more commonly used definitions [14]. However, similar methods and definitions of injury were used in the studies conducted by Clarsen et al. [5, 13] which is why the prevalence in the present study indeed needs to be considered high. Clarsen et al. [13] concluded that their new approach offers several advantages over standard methods, particularly as it allows for the use of a broad definition of injury and a means of quantifying injury severity that is not dependent on time loss. One disadvantage of the time-loss definition might be that one athlete may elect to continue playing floorball, while another player would stop playing with a similar injury. The report from one player may, therefore, result in the recording of an injury, while another will not. This problem might be rather common as overuse injuries often do not keep the athletes from participating in training or matches. The OSTRC may therefore be a better alternative for studies of overuse problems in sport. One likely explanation for the high injury prevalence in the present study might be that parents of players with symptoms that already existed before the start of the study were more likely to participate in the study than parents of players with no complaints. Further, reported injuries from the questionnaire were not followed up by any medical professionals, and the complaints were neither diagnosed nor confirmed. This may have contributed to an over-reporting of injuries. Overuse injuries and pain problems are often chronic with periods of remission and exacerbation [14]. Therefore, a best-case injury scenario in the present study was calculated, where a total of 33 injuries were found. In future studies we recommended that reports of complaints be followed up by a medical professional in order to yield more reliable data.
The most common injury locations were the knee and the foot. This is in line with previous reports regarding overuse sport injuries in children and adolescents [8, 11]. In addition, other studies focusing on adult floorball players have also recognized the knee as the most common location of overuse injury [2, 5]. For example, Pasanen et al. [2] found that, among adult floorball players, the most common location of overuse injury was the knee, followed by the lower leg and the lower back. In the present study, complaints of the lower leg were limited. The prevalence of both lower leg and hip/pelvis injuries was much lower compared to the prevalence of knee and foot injuries. One explanation for the fact that injuries to the knee and foot were so much higher than injuries to the lower leg and hip in the present study might be that these anatomical areas (knee and foot) are more exposed to injuries due to problems specific to youth. The anatomy of youth with respect to the occurrence of a growth plate makes their injury patterns dissimilar from those seen in adults. Athletes younger than 14 seem to incur many injuries in training and sustain more growth-related overuse disorders [21]. Injuries such as Osgood-Schlatter (OSD) and Sever disease are common causes of knee and heel pain respectively in active youth [22, 23]. These conditions are related to growth and development and often occur in relation to overuse syndromes and are usually seen in children aged between 8 and 15 years [21]. The players in the present study consisted of boys and girls with an average age of 11. Thus, the participants in the present study are most certainly at risk of both Sever and OSD and some of the complaints might be due to these syndromes. However, no definitive conclusions could be made due to injury registration methods. One can argue that overuse injuries have little relevance since the conditions are often benign and do not cost as much as traumatic injuries. Still, pain during growing years affects children, can cause more severe injury, and might be a predictor for future pain [24]. Pain might also have consequences for the children’s quality of life now and in the future [10].
Before the start of the present study, there was no translated version of the questionnaire available, so this was done by the author (SB). The original OSTRC Overuse Injury Questionnaire consists of questions regarding the shoulder, lower back, and knee [13]. The intention of the original authors was to create a questionnaire that could be applied to any overuse injury problem in any area of the body. The questionnaire has been shown to be valid and have a high internal consistency [13]. In the present study, the questionnaire was used for the hip/pelvis, knee, lower leg, and foot in order to fit the purpose of the present study. The translated version was discussed by both authors (SB and SRA). Moreover, the questions, in the present study were modified in order to fit this study, since the parents were supposed to answer the questions. The strong correlation between the items in the questionnaire, as shown in the study of Clarsen et al. [13], was even confirmed in the pilot test in the present study, and promising results of the test-retest were also found.
Studies with similar methods of injury registration have reported a high response rate, over 90% during the course of the study [8, 13, 25]. In the present study the response rate decreased from 91% at the first dispatch to 63% at the last. A contributing factor was probably that, in the context of the third questionnaire dispatch, a new separate information letter to the player was sent out, asking to complement the consent with the permission for continuing participation in the study. This may have led to some uncertainty as to whether or not players’ participation would continue if they had not sent in their consent forms. This may be seen as a source of error in the present study. Other limitations are the small sample size (n=57) and that data was collected monthly. Weekly reports of injuries decrease the risk of recall biases [14], and a higher degree of recall biases is therefore expected than would have been the case if data had been collected more frequently.
CONCLUSION
In conclusion, the present study indicates that overuse injuries seem to be a common problem for young floorball athletes. The knee and foot appear to be the most common locations for overuse injuries in the LE. The current study also demonstrates that injuries can be recorded by athletes, coaches, parents or other untrained individuals. This may be advantageous in the field in that injuries in young and recreational athletes can be documented where no medical expertise is available. In spite of the limitations of the study design, our findings suggest that monitoring training loads among youth floorball players is an urgent priority. Prospective analyses of different mechanisms for overuse injury in youth athletes and the relation to growth-related overuse disorders is desirable.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
Declared none.

