All published articles of this journal are available on ScienceDirect.

'Food First', Not 'Food Only' in Competitive Sports: A Mini-Review
Abstract
The use of supplements is commonplace in competitive sports. Nevertheless, sports nutrition experts keep reminding athletes to focus on a balanced basic diet with ‘natural foods‘, and not to overestimate the benefits of dietary supplements. However, depending on an individual’s training load, competition schedule, or health situation, a ‘food only‘ strategy may not be an adequate means to provide the energy and nutrients needed to win a competition. Therefore, a ‘food first‘ strategy is recommended . This approach endorses the personalized usage of certain dietary supplements (e.g., sports foods, immune modulators, performance enhancers) in specific situations in addition to a balanced basic diet. In this mini-review, we describe the circumstances in which dietary supplements can be considered ergogenic, and what kind of risks may be associated with their use.
1. INTRODUCTION
Competitive athletes are supposed to train efficiently, get enough sleep/relaxation, and eat according to their specific needs. The expectations imposed by sports nutrition experts alone are high and require a great deal of discipline and commitment. It is inevitable that athletes occasionally feel overwhelmed or deviate from an intended diet plan for various reasons (e.g., food intolerance or taste aversion). This, in turn, is often accompanied by a desire to undo ‘nutritional sins‘ by taking dietary supplements. In addition, the marketing strategies of manufacturers nurture hopes of enhancing performance through supplementation [1].
There are many reasons for taking dietary supplements, and experts estimate that 50-100% of all competitive athletes worldwide use at least one product per day [2].
In a cross-sectional study of 778 Dutch competitive athletes (407 male, 371 female), 97.2% had used supplements at some time during their sports career, and 84.7% during the last four weeks [3]. Recent studies from Spain evaluated similar proportions of supplement users and indicated that supplement consumption increases with competition level, suggesting that men tend to consume more supplements than women [4] and older athletes have higher consumption rates than younger ones [5].
The aim of this mini-review is to highlight scenarios in which nutritional measures alone may be insufficient to gain a decisive advantage over an opponent, and where the evidence-based use of dietary supplements may be beneficial.
2. METHODOLOGY
In September 2024, a systematic literature search was conducted using the MEDLINE database (via PubMed). The initial search with the keywords 'food first' AND “sports nutrition” yielded only n = 5 results (2019–2023). To broaden the scope, the keyword “food first” alone was used, resulting in n = 96 hits. After the abstract screening, n = 12 full-text articles in English were selected. A subsequent unsystematic search was performed to identify relevant position papers, systematic reviews, meta-analyses, and randomized controlled trials (RCTs) addressing nutritional recommendations and supplementation strategies for competitive athletes, with inclusion limited to supplements classified as Group A by the Australian Institute of Sport (AIS). The same procedure was applied to n = 7 position papers from the German Nutrition Society, originally written in German.
3. RESULTS/DISCUSSION
3.1. Background and Definitions
3.1.1. Food First
A balanced basic diet, as depicted for different training loads (easy, moderate, hard) in The Athlete’s Plate® [6, 7], is undoubtedly an indispensable prerequisite for success in competitive sport [8]. In line with this, the term ‘food first‘, first mentioned in 2019 [9], implies that whenever possible, from a practical point of view, an athlete should try to meet his water, energy, and macro-/micronutrient requirements with everyday food and drinks, and not by using dietary supplements. The main reason for this ‘food over supplement‘ concept is that natural food sources provide many different nutrients and other functional ingredients not in isolated form but combined, which has positive effects on the gut microbiome, inflammatory processes, immune tolerance, and neuroprotection [10]. In addition, meals have both a psychological and, within a community, a social component, and they can positively influence mood [11]. As important as a balanced basic diet is, 'food first' should not be interpreted as 'food only'. In some cases, strict avoidance of dietary supplements is neither practical nor advisable [12]. A 'food only' strategy could lead to a reduction in performance under certain circumstances (e.g., due to insufficient time to consume the required amount of food), and some individuals may miss out on a small but significant performance benefit by not using dietary supplements. Several factors can make a 'food only' approach debatable in competitive sports, which are as follows:
-Training sessions, along with school or work commitments in the case of a dual career, can take up a significant amount of time, leaving insufficient time to prepare and consume bulky, wholesome meals frequently enough to provide the body with adequate energy and nutrients.
-Consuming food shortly before and during exercise of moderate to high intensity can cause gastrointestinal distress, and it is sometimes impractical to take the appropriate food to a competition.
-Meals may be skipped after exercise of long durations due to a lack of appetite.
-Specific nutrients can be provided more quickly by sports foods, which is useful when there are less than 24 hours before the beginning of the following vigorous training bout or competition.
-Certain foodstuffs or food groups may be avoided, and/or energy intake may be restricted for health (e.g., food intolerances), ethical (e.g., veganism), religious (e.g., haram foods, Ramadan), performance-related (e.g., weight loss), or other reasons (e.g., anorexia athletica).
-Food choices may be limited when traveling, or there may be concerns regarding food hygiene.
-A detected nutrient deficiency should be addressed quickly, which is not always feasible through food alone (e.g., vitamin D in indoor sports).
-Depending on the immune status, a nutrient intake above the dietary reference value may be advisable (e.g., vitamin C during the cold season).
-The content of food components can fluctuate (e.g., nitrate levels in vegetables), leading to potential under- or over-dosage.
-Some ergogenic substances cannot be provided in sufficient amounts through everyday food without also consuming excessive amounts of protein, fat, or cholesterol (e.g., creatine in meat).
-Contamination of food with banned substances cannot be ruled out completely (e.g., the anabolic steroid clenbuterol in meat [13]).
3.1.2. Dietary Supplements
According to the International Olympic Committee (IOC) consensus statement 2018, a dietary supplement is defined as “a food, food component, nutrient, or non-food compound that is purposefully ingested in addition to the habitually consumed diet with the aim of achieving a specific health and/or performance benefit” [14]. Unlike food and drugs, dietary supplements containing micronutrients, probiotics, or ergogenic substances are not subject to state-regulated control [15].
3.1.3. Supplement Categories
The ABCD classification system of the Australian Sports Commission [16] subdivides sports foods and supplement ingredients into four groups according to scientific evidence and other practical considerations that determine whether a product is safe, permitted, and effective in improving sports performance (Table 1). The grade of scientific evidence is based on the results of meta-analyses and RCTs, which are summarized in the “practitioner fact sheets” available for download from the Australian Sports Commission website [16].
For “Group A” dietary supplements—sports foods, medical supplements, and performance supplements—there is strong scientific evidence supporting their application in specific sports situations using evidence-based protocols. This means that the supplement must align with the intended purpose and that the dosage should be validated in clinical trials. Additionally, individual differences in response to supplements (e.g., high/low responders) and tolerance (e.g., side effects) must be considered. A key prerequisite for the additional benefits of a dietary supplement is that training schedules, sleep/relaxation time, and performance-oriented nutrition are already well-established.
The following sections will discuss only the supplements from “Group A” and vitamin C (“Group B”). Substances not mentioned either have limited evidence (“Group B”, e.g., collagen, carnitine, ketones) or no evidence (“Group C”, e.g., leucine, magnesium, HMB) regarding their effectiveness on performance, muscle function, or health optimization. Group D includes doping-relevant substances.
| Group A1: | Group B2: | Group C3: | Group D4: |
|---|---|---|---|
|
Sports foods: - sports drinks - electrolytes - isolated proteins - sports gels - sports bars - sports confectionary - mixed macronutrient supplements Medical supplements: - multivitamins - vitamin D - calcium - iron - zinc - probiotics Performance supplements: - caffeine - creatine - dietary nitrate - β-alanine - sodium bicarbonate - glycerol |
Fruit-derived polyphenols: - whole fruit (powder), juice, concentrate, and extract of cherries, berries, blackcurrant, pomegranate, red grapes, etc. Antioxidants: - vitamin C Tastants: - menthol - pickle juice - quinine Other: - collagen - fish oil (EPA/DHA) - carnitine - ketones - N-acetyl cysteine - curcumin |
- branched-chain amino acids/leucine - tyrosine - vitamin E - magnesium - phosphate - β-hydroxy-β-methylbutyrate (HMB) - alpha lipoic acid - prebiotics - other |
Stimulants: - ephedrine - strychnine - sibutramine - 4-methylhexan-2-amine - 1,3-dimethylbutylamine - other herbal stimulants Prohormones and hormone boosters: - DHEA - 4-androstenedione - 19-norandrostendione - other prohormones - tribulus terrestris - maca root powder GH-releasers and ‘peptides‘: - GHRP1 & GHRP2 - CJC1293 & CJC1295 Beta-2 agonists: - higenamine Selective androgen receptor modulators: - ostarine - andarine - ligandrol Metabolic modulators: - cardarine (GW1516) Other: - colostrum |
3.2. Food vs. Supplements in Sports
3.2.1. Water, Energy, and Macronutrients (sports foods)
3.2.1.1. Water Supply
Since dehydration compromises thermoregulation and can cause impairment in performance, it is crucial to compensate for the water and sodium loss caused by sweating during training and competition as fast as possible. However, this does not necessarily require the use of commercial isotonic sports drinks. As stated in the position paper of the German Nutrition Society on fluid replacement in sports, mineral water and fruit juice spritzers before and during exercise, as well as milk-based beverages and alcohol-free beer after exercise, are also recommended [17].
3.2.1.2. Energy Supply
Serious and/or prolonged low energy availability (LEA) can negatively impact numerous physiological and psychological systems, thereby impairing performance outcomes, training adaptations, and overall health status [18]. Liquid meals offer a compact source of varying amounts of protein, carbohydrates, and micronutrients for use in situations where consuming whole foods is difficult or when appetite is suppressed [16]. However, whenever possible, energy needs should be met through regular meals [19].
3.2.1.3. Carbohydrate Supply
Since decreasing blood glucose levels are associated with fatigue, it is essential to begin prolonged, moderate-intensity exercise, as well as activities involving repeated bouts of vigorous exercise, with high concentrations of glycogen in the muscles and liver. Consuming carbohydrates during exercise delays muscle glycogen depletion and stabilizes blood glucose levels, thereby supporting or enhancing performance. Providing carbohydrates immediately after exercise accelerates glycogen resynthesis and promotes recovery. According to the position paper of the German Nutrition Society on carbohydrates in sports nutrition, carbohydrate providing sports foods are considered appropriate in the following situations [20]:
1 Carbohydrate loading before (ultra-)endurance competitions (10–12 g/kg/day), as large amounts of carbohydrate-rich foods such as pasta, rice, bread, or potatoes can place a heavy strain on gastrointestinal capacity.
2 Consumption of highly concentrated glucose, fructose, and dextrins before and during intense exercise lasting longer than 90 minutes, since ingesting the necessary amount of carbohydrates to delay fatigue (30–120 g/h) in the form of fruit juice, dried fruit, granola bars, or toast may cause gastrointestinal distress and pose logistical challenges—particularly during activities, such as swimming or running.
3 Refueling after long-duration endurance activities (guideline: 1 g/kg/hour for four hours), as appetite is generally low post-exercise.
In order to quickly provide glucose, energy bars, carbohydrate gels, sports confectionery, and sports/recovery drinks can be useful. Bananas are also an excellent source of glucose in a natural ‘wrapping‘ (a large ripe banana provides approx. 30 g of carbohydrates). However, the absorption of glucose from sports drinks and gels is faster [8, 20, 21].
3.2.1.4. Protein Supply
Due to its role in facilitating muscle building and repair in strength and power sports, and because of increased amino acid oxidation during intense endurance exercise, an adequate protein intake is essential across all sports disciplines. According to the position paper of the German Nutrition Society on protein intake in sports, isolated protein supplements may be beneficial in the following situations [22]:
1. While traveling, as it may be difficult to consume up to 1.6 g/kg/day of protein, the amount required to support net muscle protein synthesis, distributed over several servings of 20 to 25 g each.
2. Before bedtime, when 30–60 g of casein is recommended; for example, consuming 40 g of casein would require the intake of approximately 1,175 ml of skimmed yogurt (660 kcal) or 1,025 ml of skimmed milk (360 kcal).
Compared to protein-rich whole foods such as cheese, meat, fish, egg whites, or tofu, whey protein concentrate—or alternatively, soy protein isolate for those following a plant-based diet—provides amino acids in a more easily digestible and ready-to-consume form.
It is important to note that sports foods should not be consumed for convenience. They are supposed to complement, not replace, a balanced diet rich in whole foods. Whole food provides a variety of essential nutrients, bioactive compounds, and fibre that supplements may lack [8, 21].
3.2.2. Micronutrients and Probiotics (medical supplements)
Adequate intake of vitamins and minerals is essential for both health and performance, as is the maintenance of a diverse gut microbiota. The use of so-called medical supplements may support an athlete’s performance and well-being in the following situations: when a (subclinical) micronutrient deficiency has been diagnosed, and potentially even in the absence of an identifiable deficiency, if enhanced immune tolerance is needed to combat infectious diseases.
3.2.2.1. Micronutrient Deficiency
Vitamins and minerals are crucial for an athlete’s health and physical performance, and no single micronutrient is more important than others [23]. In a recent study of 111 German elite athletes (61 female, 50 male) performing in different disciplines, micronutrient deficiencies were detected for vitamin D, magnesium, iron, and selenium [24]. As described in the position paper of the German Nutrition Society on vitamins and minerals in sports nutrition [25], a suboptimal micronutrient status is usually due to an unbalanced diet or low energy availability, but increased losses or reduced absorption can also play a role. As these essential nutrients are involved in the regulation of the metabolic body’s functions, such as energy production, muscle growth, and recovery, a (sub)clinical deficiency can have a direct (e.g., reduced training capacity in iron deficiency anemia) or indirect (e.g., increased stress fracture risk in hypocalcemia) negative effect on performance.
An exemplary micronutrient at risk of deficiency in competitive athletes is iron, a trace mineral involved in energy metabolism, oxygen transport, and cognitive function. In a recent study of 1190 German competitive athletes (783 males, 407 females), 19.7% were afflicted with iron deficiency associated with reduced athletic performance, with a higher prevalence in females and younger athletes [26]. Factors such as inadequate iron intake or absorption, as well as increased iron losses due to exercise-induced sweating, hematuria, and gastrointestinal bleeding, elevate the risk of iron deficiency, with or without anemia. Regular monitoring of iron status through blood tests, including serum ferritin and hemoglobin levels, is essential for early detection. In cases of significant deficiency that cannot be corrected through dietary intake, such as the consumption of iron-rich foods (e.g., liverwurst, meat, beans, sesame, pistachios, and cashews) combined with absorption enhancers like vitamin C, while avoiding inhibitors such as phytates and calcium, iron supplementation is required. This should be administered either orally (100–200 mg/day) or intravenously under medical supervision [27].
When a micronutrient deficiency cannot be corrected quickly enough through regular food intake, supplementation is indicated. The dosage and duration of supplementation should be determined in consultation with a healthcare professional to avoid side effects and interactions with medications. After supplementation, the diet should be adjusted to meet nutrient requirements as closely as possible to prevent the recurrence of the deficiency. A continuous intake of micronutrients in excess of physiological needs, through single or multivitamin/mineral supplements, is not advisable [28]. Such excess has no proven benefit for performance and may lead to intake levels above the Tolerable Upper Intake Level (UL), or, in the case of contaminated products, may result in violations of anti-doping regulations.
3.2.2.2. Infection Defense
As in the general population, athletes experience an increased incidence of respiratory infections during the cold season and gastrointestinal infections when traveling [29]. Other risk factors include psychological stress and poor sleep. In addition to macronutrients (proteins and carbohydrates for immunoglobulin synthesis), antioxidative micronutrients, as well as the gut microbiome, are involved in a variety of immunological processes.
Since immune function in athletes is generally not impaired, it is not surprising that intervention studies involving supplementation with vitamin A or vitamin E—intended to enhance immune resistance and prevent infections—have not been successful. In fact, some studies reported a negative impact on training adaptations [30]. Therefore, an alternative approach explores whether immune tolerance can be
| Probiotics (Lactobacilli, Bifidobacteria) |
|---|
| Live probiotic bacteria, naturally found in fermented foods such as yogurt, kefir, kombucha, and sauerkraut, positively affect the intestinal barrier and contribute to stabilizing the immune system when certain subspecies are consumed daily in sufficient quantities (1010 colony-forming units) for at least two weeks. A Cochrane review suggests that probiotic supplements may reduce the incidence of upper respiratory tract infections (URTI) in adults, including athletes, by 25%, and shorten the duration of URTI episodes by an average of 1.2 days [36]. Additionally, a meta-analysis indicates that probiotics can alleviate gastrointestinal symptoms during high-intensity exercise, travel, and antibiotic-associated diarrhea [37]. Aside from flatulence, no significant side effects have been observed. |
| Vitamin D (cholecalciferol) |
| Vitamin D, an essential fat-soluble vitamin found in fatty fish, margarine, butter, egg yolk, milk, and dairy products, has anti-inflammatory properties and plays a key role in regulating immune functions, such as the expression of antimicrobial peptides (AMP). A meta-analysis has shown that daily supplementation with vitamin D can reduce the risk of developing upper respiratory tract infections (URTI). However, the protective effect is more pronounced in individuals who are vitamin D deficient (plasma 25[OH]D3 < 25 nmol/l) compared to those who are adequately supplied [38]. Vitamin D deficiency typically occurs when there is insufficient skin exposure to UV radiation over a prolonged period (e.g., low UV index in winter or year-round indoor training), as dietary intake alone is often inadequate to meet requirements. To ensure safe levels of vitamin D, supplementation of 20-50 µg/d (800-2000 I.U./d) is recommended, with a daily maximum of 100 µg/d (4000 I.U./d) to avoid side effects such as stomach pain, nausea, and reduced appetite [21]. |
| Vitamin C (ascorbic acid) |
| Vitamin C, an essential water-soluble vitamin found in high concentrations in fruits and vegetables, has antioxidant properties. It scavenges reactive oxygen species (ROS), which can stimulate the synthesis of pro-inflammatory cytokines, leading to tissue damage. According to a meta-analysis, daily supplementation of ≥1000 mg of vitamin C over several weeks can reduce the severity of the common cold by 15% and shorten the duration of severe symptoms (but not mild ones) by 26%, with a greater effect observed in males compared to females [39]. However, long-term supplementation exceeding 1000 mg/d is generally not recommended, as such high doses of vitamin C can cause diarrhea. Additionally, like high-dose vitamin E, vitamin C may have a prooxidative effect, potentially increasing lipid peroxidation and impairing training adaptation. This occurs by suppressing the transient formation of ROS during aerobic exercise, which reduces the ROS-induced activation of two redox-sensitive signaling pathways (NF-κB and MAPK) that are involved in the positive muscle response to training stimuli [40]. |
| Zinc lozenges |
| Zinc ions are thought to reduce the docking of viruses to receptor molecules in the throat when administered as a lozenge. According to a Cochrane review, zinc gluconate, orotate, or acetate—whether taken orally, intranasally, or as lozenges—has no preventive or therapeutic effect on the common cold in adults or children [41]. However, several shortcomings in this Cochrane review have been pointed out by the authors of a previous meta-analysis on zinc lozenges. This analysis concluded that 15 mg of elemental zinc taken five times per day at 3-hour intervals can shorten the duration of a common cold in adults by 30-40%, provided that the treatment is started no later than 24 hours after the appearance of the first symptoms [42]. Side effects of sucking zinc lozenges include a bad taste in the mouth and nausea. The lozenges should be discontinued immediately after symptoms subside, as zinc inhibits copper absorption. |
improved by supplementing with specific micronutrients or probiotics, as listed in Table 2. The goal is to modulate the immune system in a way that prevents excessive immune reactions, thereby reducing the severity and duration of illness [31].
A general objection to the use of the potentially immune tolerance-enhancing supplements listed in Table 2 is the moderate level of evidence supporting them, primarily due to study limitations such as self-reporting bias. To eliminate placebo effects and account for the specific demands of competitive sports, future studies should be not only randomized and controlled [32, 33], but also conducted on highly trained male and female athletes [34, 35], with a focus on clinically relevant immune parameters [36-42].
3.2.3. Ergogenic Substances (performance supplements)
Supplements marketed as so-called ‘performance enhancers‘ are intended to improve performance capacity, promote training adaptation, and/or accelerate regeneration in athletes. Depending on the specific goal, they are either applied once before a competition or continuously over several weeks to months in preparation for an event.
A dietary supplement is considered ergogenic if RCTs conducted on athletes under conditions closely resembling real-world settings demonstrate improvements in endurance or strength/power performance beyond the effects of training alone. Table 3 summarizes the mechanisms of action, areas of application, food sources, suggested dosages, and potential risks or adverse effects of the six dietary supplements classified under “Group A” by the Australian Institute of Sport [16].
The information on dosage is derived exclusively from meta-analyses and RCTs. Although there is a broad scientific consensus [12, 14, 31, 43, 44], this information is not intended to be a general intake recommendation. If at all, the choice of a supplement and its dosage needs to be personalized. In addition, the positive and negative effects on performance and well-being should be recorded during training, and the risk of contamination with banned substances must be kept to a minimum.
3.3. Risks associated with Supplement Intake
Apart from the fact that well-marketed products do not always meet user expectations and can lead to disappointment, there is also a risk of nutritional imbalances when relying too heavily on supplements, as well as the risk of violating anti-doping regulations in competitive sports. Such violations can result in disqualification and the forfeiture of medals, points, and prizes [45]. Dietary supplements may contain undeclared banned substances (“Group D”, e.g., ephedrine, DHEA, ostarine). Contamination can occur unintentionally during the manufacturing process, or a banned substance may be intentionally added without being disclosed on the label or may be listed under a different name. A recent study conducted in the Netherlands found that the prevalence of undeclared doping substances in commercial sports nutrition supplements can be as high as 38% [46].
A relatively good level of protection from unintentional doping can be achieved by using dietary supplements from reputable manufacturers and checking for third-party testing on websites like e.g., www.bscg.org (USA) or www.koelnerliste.com (Germany). For proof of unintentional doping, it is advisable to store approx. 30 g of each dietary supplement used [47].
| Modes of Action | Areas of Application | Food Sources (‘food first‘) | Suggested Dosages | Risk/adverse Effects of Supplementationa |
|---|---|---|---|---|
| Caffeine: adenosine receptor antagonist acting as a central nervous stimulant in numerous situations (most commonly used supplement in endurance sports) | ||||
| - alertness and vigilance ↑ - sensation of exertion/pain ↓ - neuromuscular function ↑ - performance (endurance, strength/power, speed, jump) ↑ |
- before and during endurance exercise lasting > 60 minutes - before exercise lasting < 60 min as an ‘energy booster‘ in case of fatigue |
- naturally present in foods such as coffee, tea and coke - content subject to natural fluctuations and depending on the type of preparation (e.g. 15-250 mg/serving in coffee drinks) → under- as well as overdosage possible |
- 3-6 mg/kg, 5-60 min before a competition - 1-2 mg/kg together with carbohydrates towards the end of intensive endurance exercise - added to various sports drinks, gels, bars and chewing gum |
- dosages > 4 mg/kg associated with nervousness, palpitations, gastrointestinal discomfort, confusion, disturbed sleep, etc. - 5-30 g caffeine lethal |
| Creatine provides energy in the form of creatine phosphate for short, high-intensity exercise bouts (most commonly used supplement in strength/power sports) | ||||
| - capacity to perform maximum or repeated high-intensity exercise ↑ - muscle growth ↑ (indirectly via increased training capacity) - strength, peak/mean power, speed ↑ (indirectly via increased training capacity) - muscle atrophy due to immobilization after injury ↓ |
- weight lifting and sprint performances lasting < 2.5 min - to support regeneration and rehabilitation - vegan/vegetarian athletes benefit more from supplementation than omnivorous athletes |
- supply via food not sufficient to achieve a performance benefit (3-6 g creatine per kilogram of raw meat, significantly less in cooked meat) |
- loading phase: 4 x 5 g/d for 5-7 days as creatine monohydrate - maintenance phase: 3-5 g/d - increased muscular uptake with simultaneous intake of 50 g carbohydrates and proteins |
- ~1-2 kg weight gain due to water retention - possibly gastrointestinal discomfort, which can be reduced by taking smaller doses throughout the day - possibly increased creatinine level - no risk for the kidneys with long-term use (< 30 g/d for 5 years) |
| Nitrate increases the availability of nitric oxide, which plays an important role in the regulation of blood pressure and blood flow. | ||||
| - vasodilation ↑ → oxygen transport to the muscles ↑ - mitochondrial respiration ↑ → improvement of exercise economy - in recreational athletes only: endurance capacity ↑ - contraction of type II muscle fibres ↑ |
- before submaximal exercise lasting 4-30 min - strength, sprint, and high-intensity interval training - hypoxia/altitude training - in highly trained athletes less pronounced effect |
- naturally present in green leafy and root vegetables (sufficient amounts) - content subject to natural fluctuations (e.g., 100-425 mg/100 g spinach, 100-275 mg/100 g lettuce, 65-180 mg/100 g beetroots) - veggies too high in fibre to eat before the competition (gastrointestinal distress) |
- 300-550 mg, 2-3.5 h before a competition (no significant difference whether 1 or 15 days long) - 400 mg are provided by 500 ml beetroot juice or 70 ml beetroot shot |
- gastrointestinal discomfort and change in color of stool/urine after consumption of (highly concentrated) beetroot juice/shots - reduced uptake of iodine into the thyroid - potential carcinogenic effect of nitrosamines formed in the stomach |
| β-Alanine: increases the muscle carnosine concentration and thereby the intracellular buffer capacity for acids (lactate), which delays fatigue | ||||
| - anaerobic-lactacid ATP-synthesis ↑ - speed/power ↑ - work capacity ↑ |
- high-intensity continuous or intermittent exercise lasting 0.5-10 minutes - endurance exercise with intermediate sprints and final spurt - in highly trained athletes less pronounced effect |
- supply via food too low (200 g chicken breast increased plasma levels like 800 mg supplement) - carnosine from food (e.g. meat/fish) is broken down to β-alanine and histidine in the small intestine → no effect on muscle carnosine concentration |
- 65 mg/kg/d for 4-12 weeks, usually 4 daily doses of 0.8- 1.6 g/kg each at intervals of 3-4 h |
- single doses > 0.8 g associated with tingling in the face, neck, and back of the hand - high/low responders - intakes ≤ 4 months safe |
| Sodium bicarbonate increases the hydrogen carbonate concentration in the blood and, thereby, the humoral pH value, which slows down the intracellular acidification and the onset of fatigue | ||||
| - muscular efflux of H+ ions ↑ - anaerobic-lactacid ATP-synthesis ↑ - speed/power ↑ - work capacity ↑ |
- before high-intensity exercise lasting 1-10 minutes - before endurance exercise up to 1 h with sprints |
- a high-carbohydrate/low-protein diet for several days also increases the pH value in blood and muscles, but to a lesser extent than supplements - baking soda (very salty taste) together with a carbohydrate-rich meal and plenty of fluids can be tried |
- 200-500 mg/kg, 1-3 h before a competition - to date, there is too little empirical data on the MaurtenTM Bicarb System to recommend this hydrogel product [33] |
- gastrointestinal discomfort like abdominal pain, diarrhea, nausea, vomiting - elevated urinary pH value for a few hours (important for anti-doping controls) |
| Glycerol enables a higher retention of fluid in the body by increasing water reabsorption in the kidneys, which has a positive effect on thermoregulation | ||||
| - tolerance of sweat losses ↑ when used before sports - regeneration ↑ when used after sports - fluid balance ↑ when used after weight cutting (= intentional dehydration in weight class sports) |
- before prolonged intensive exercise in hot/humid environment - sports with several starts on consecutive days - after weigh-in in combat sports - limited access to drinks |
- supply via food too low (basic structure of triglycerides/ additive E422) |
- 1,2 g/kg, 1.5-3 h before a competition - ingestion together with water (25 ml/kg) and sodium (3 g/l) |
- gastrointestinal discomfort like stomach pain, nausea, flatulence, laxative effect - weight gain due to hyperhydration - risk of development of hyponatremia in ultra-endurance sports |
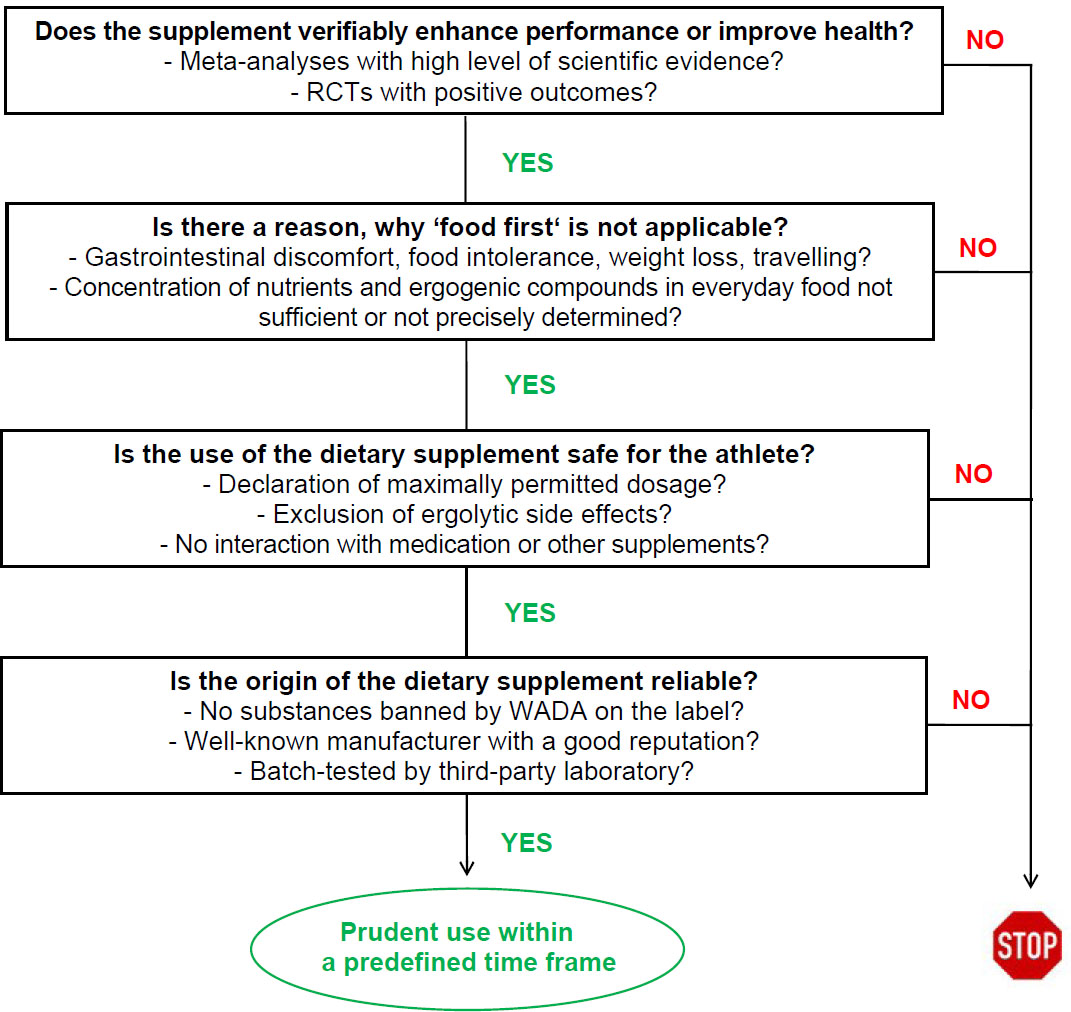
Flowchart designed to determine whether or not to use a dietary supplement in performance sport [14].
Some dietary supplements contain higher or lower levels of ingredients than the amounts declared on the label [14]. If the maximum permitted concentration is exceeded, overdose-related effects cannot be ruled out; if the concentration is lower than this, the product may be ineffective [48].
3.4. Decision Tree
Since a few supplements can enhance health and/or performance, it may be warranted in specific situations to consider an evidence-based use. It is recommended that the athletes collaborate with an expert team of a nutritionist and a sports physician and apply the decision tree as shown in Fig. (1). As part of a consensus statement of the International Olympic Committee [14], the decision tree was designed to help athletes decide whether or not to take a dietary supplement. In general, supplements should first be tested in training and during less important events before they are used in important competitions.
3.5. Special Considerations
3.5.1. Female Athletes
Despite the progress towards gender equality in international competitions, scientific studies focussing on establishing specific nutritional recommendations for female athletes are scarce.
The International Society of Sports Nutrition and a systematic review have outlined dietary and supplementation strategies tailored to improve sports performance, recovery, and health in female athletes, considering their unique hormonal profiles [35, 49]. The evidence-based recommendations can be summarized as follows: The primary nutritional goal should be to achieve adequate energy intake, with an emphasis on the timing of meals in relation to exercise. The diet should be high in carbohydrates, and protein intake should be evenly distributed across the day, with doses of approximately 25 grams every 4 hours. Additionally, the use of specific sports foods (e.g., carbohydrates, proteins, or their combination), micronutrients (e.g., iron), and performance supplements such as caffeine, creatine, nitrate, or β-alanine may be beneficial in certain situations, positively influencing sports performance and/or health status in female athletes [35, 49].
3.5.2. Young Athletes
The increasing participation of young individuals in sports necessitates evidence-based nutritional strategies supporting growth, energy metabolism, and overall athletic achievement [50]. In a personalized approach with emphasis on a balanced basic diet, it must be ensured that energy and macronutrient demands are met. In addition, the micronutrient status, especially of vitamin D, calcium, iron, zinc, and vitamins C, E, B6, B12, and folate, has to be monitored proactively through regular assessments in order to tailor dietary strategies accordingly. Commonly discussed supplements for young athletes include vitamin D, iron, omega-3 fatty acids, protein isolates, and creatine. However, supplements should be used cautiously, and a healthcare professional or dietitian should be consulted before incorporating them into a daily routine. Balancing nutritional needs with practical considerations, such as school schedules and training times, is essential. Planning meals in advance and providing easily accessible snacks can help successfully integrate sound nutritional practices into an athlete’s lifestyle [50].
3.5.3. Athletes Adhering to Plant-based Diets
Plant-based diets, mainly consisting of plant foods, such as fruits, vegetables, potatoes, legumes, and oilseeds, are growing in popularity as they are considered healthy and environmentally sustainable [51]. However, it can be challenging to ingest sufficient amounts of essential amino acids, long-chain omega-3 fatty acids, vitamin B12, iron, calcium, iodine, and zinc [52]. In order to clarify the impact of a plant-based diet on variables of aerobic and anaerobic sports performance and health, a meta-analysis and a systematic literature review were conducted [53, 54]. Compared to omnivorous athletes, the overall effects on performance and health were not significantly different, even though the Body Mass Index (BMI) of the adherents of the plant-based diets was reduced [53, 54]. Due to study limitations such as substantial variability among the experimental designs, aims, and outcomes, further research is required, especially in elite athletes [51].
CONCLUSION
In competitive sports, a ‘food only‘ approach seems inappropriate. ‘Food first‘ should be the preferred nutrition strategy, although there is no agreed definition and often limited consideration of the implications. ‘Food first‘ means that athletes should prioritize a balanced diet as the foundation of their nutritional strategy and use supplements to complement rather than replace whole foods [19]. In other words, “Where practically possible, nutrient provision should come from whole foods and drinks rather than from isolated food components or dietary supplements“ [31]. Athletes are explicitly discouraged from using over-the-counter supplements—either individually or in combination—without a clinical diagnosis of nutrient deficiency and without consulting the decision tree of the International Olympic Committee due to the potential risks of unbalanced nutrient provision, undesired interactions, side effects, and increased doping risk (Fig. 1) [14].
The ‘food first’ concept allows athletes to incorporate dietary supplements into their diet plan, particularly sports foods and essential micronutrients, to maintain or restore performance capacity in the event of increased requirements or (sub)clinical deficiencies. Occasionally, ergogenic substances may also be used to specifically promote performance. When dietary supplements are used in a personalized manner, they can help achieve nutritional goals, support intense training, facilitate recovery, prevent injuries and infections, and potentially provide a small but meaningful performance advantage. However, dietary supplements are not a substitute for performance-oriented nutrition. ‘Food over supplement‘ must always be the basic principle in applied sports nutrition, and athletes need to be educated accordingly.
AUTHORS‘ CONTRIBUTIONS
The author confirms sole responsibility for the following: A.S.: Study conception and design, data collection, analysis and interpretation of results, and manuscript preparation.
LIST OF ABBREVIATIONS
| RCTs | = Randomized Controlled Trials |
| ROS | = Reactive Oxygen Species |
| UL | = Tolerable Upper Intake Level |
| URTIs | = Upper Respiratory Tract Infections |
ACKNOWLEDGEMENTS
Declared none.
REFERENCES
http://dx.doi.org/10.5960/dzsm.2020.453
http://dx.doi.org/10.5960/dzsm.2020.456
http://dx.doi.org/10.5960/dzsm.2020.450
http://dx.doi.org/10.5960/dzsm.2020.455

