All published articles of this journal are available on ScienceDirect.

The Effect of Body Composition on Aerobic Fitness Levels and Hemodynamic Factors in Children: A Review of Literature
Authors Info & Affiliations
Abstract
The benefits of physical activity (PA) are well established. However, the majority of children worldwide fail to meet the recommended weekly requirements for PA, which are essential for enhancing cardiorespiratory fitness (CRF) and maintaining a healthy weight for their age. The present review evaluated published work in an effort to study the effects of body composition on aerobic fitness levels and hemodynamic factors in children.
Studies were retrieved from the following databases: Cochrane Database of Systematic Reviews, PubMed (2013-June 2024), Google Scholar, Scopus, Science Direct, EBM Reviews, Current Contents, CISTI Source (2011-June 2024), Sports Discuss (2019-June 2024), and international e-catalogues. Search analysis from these periods represents recent developments, ensuring that the review reflects up-to-date understanding in the field. This helps incorporate the latest methodologies, findings, and technological advancements, and strengthens the validity of this review. The population consists of children from both industrialized and developing nations. The selected study designs were cross-sectional, longitudinal, cohort, review, and systematic review. The analysis of research entailed reading titles, abstracts, and complete texts. Following these processes, thirty articles were considered for review. The broad investigation aims to reveal the effects of body composition on aerobic fitness levels and hemodynamic parameters in preventing childhood obesity. The search strategy, as well as Medical Subject Heading (MeSH) phrases and keywords, were used to effectively route significant papers addressing childhood obesity. The relevant terms were “body composition,” “overweight,” “obesity,” “physical activity,” “heart rate,” “blood pressure,” “aerobic fitness”, “nutrition,” “cardiovascular disease,” and “children aged 10-18 years old.”
We discovered 12972 publications related to childhood obesity, hemodynamic variables, physical activity (PA), and aerobic fitness; however, 9194 articles were deleted due to duplication. The number of studies left after removing duplicates was 3778. Furthermore, 1657 articles were removed because they were not in English, 1240 articles had no full text available, and 809 articles only included abstracts. Moreover, the full text was reviewed for eligibility, which included 42 reference reviews and 18 titles. Finally, 30 articles were deemed eligible for review
The existing literature suggests that additional investigation is warranted to delineate a precise course of action for mitigating the risks associated with childhood obesity. This entails placing a heightened emphasis on the significance of children engaging in aerobic fitness activities.
1. INTRODUCTION
Obesity is increasingly impacting a number of children and adolescents worldwide, with a rising prevalence in both high-income countries as well as low-and middle-income countries (LMIC) [1, 2]. Hence, childhood obesity is associated with various health conditions, including type 2 diabetes, cardiovascular disease (CVD), respiratory problems, joint problems, poor academic performance, psychological effects, and increased premature mortality rates worldwide [2, 3]. A major component in preventing childhood obesity is engaging in physical activity (PA) [2, 3]. A considerable 80% of the pediatric population does not meet the public health standard for PA. Although the causes of childhood obesity are complex, a decline in energy expenditure and a decrease in aerobic fitness levels are regarded as one of the most significant indicators for excessive body composition (BC) in children [4, 5].
Additionally, inadequate levels of PA significantly contribute to non-communicable diseases, resulting in approximately 5.3 million deaths annually [3-5]. The World Health Organization (WHO) estimates that only 20% of adolescents worldwide participate in sufficient PA, which is a minimum of 60 minutes of physical activity 3-5 times per week [5-7]. Evidence indicates that the decreasing levels of PA play a significant role in the rising prevalence of childhood obesity [8-10]. Globally, in 2016, over 41 million children under the age of five were classified as overweight (O/W) and obese [5, 10, 11]. In southern Europe, over 40% of children under 10 years old were diagnosed with overweight or obesity, in contrast to less than 10% in northern Europe. Overall, girls were found to have a higher likelihood of being overweight or obese compared to boys (21.1% vs. 18.6%) [6-8]. Various factors have been suggested as contributors to O/W and obesity among children [11, 12]. These factors include genetics, reduced PA levels, increased sedentary behaviour (SB), excess body composition, and dietary changes [8-12].
Furthermore, lifestyle factors, such as family influences and societal attitudes, have been linked to the growing prevalence of childhood obesity and O/W in children [6, 10, 11]. Moreover, children having an excessive amount of body composition has a negative impact on their overall health, increasing their risk of developing cardiovascular diseases (CVD) as well as reducing their average life expectancy [12-16]. Hence, regular PA to improve aerobic fitness levels is one of the most recommended and effective methods for the management of childhood obesity [17, 18]. As a result, CVD remains one of the main contributors to adult mortality worldwide [17-19]. Clinical signs of CVD typically appear later in life despite mounting evidence that it begins in childhood [12, 16]. High blood pressure (HBP) in children is also a sign of poor cardiovascular health, and being overweight or obese during adolescence weakens the cardiovascular system later in life [20-22]. Low levels of fitness have been identified by The American Heart Association (AHA) as a significant risk factor for CVD [19, 20, 22]. For this reason, it is critical that children engage in aerobic fitness activities like walking, swimming, running, and cycling to lower their risk of developing CVD in the future [17, 19]. Childhood and adolescence are challenging phases characterized by rapid maturation and growth [17, 21].
Moreover, the future well-being of children is greatly impacted by the behaviors and habits that form during this period [8, 21, 22]. However, recent studies have indicated that children who participated in PA activities had significant improvements in body composition and aerobic fitness levels, further reducing the risks of childhood obesity and CVD in children [3, 14, 21]. Therefore, weight gain in children and adolescents is associated with a decline in PA [13, 22]. Despite the growing body of literature on the global problem of childhood obesity, few randomized controlled reviews have analyzed the effects of body composition, aerobic fitness levels, and hemodynamic variables among children [11, 22]. It is imperative to emphasize the relevance of aerobic fitness in relation to appropriate weight management in children as part of the prognosis of excessive body composition in children frequently [10, 18, 22]. Based on the literature, there are multiple studies that focus on each of the associations individually [14, 21], but none have attempted to bring them together. This is the novelty of this review. Therefore, this review aims to analyze the effects of body composition on hemodynamic variables, as well as aerobic fitness levels in children.
2. MATERIALS AND METHODS
2.1. Search Strategy
To analyse the literature review on the effects of childhood obesity on aerobic fitness levels and hemo- dynamic factors, a literature search was conducted on electronic search engines, including EBM Reviews, Current Contents, PubMed, Science Direct, Google Scholar, CISTI Source (2011-June 2024), Sports Discuss (2019-June 2024), Cochrane Database of Systematic Reviews, PubMed (2013-June 2024), and international e-catalogues. Search analysis from these periods represents recent developments, ensuring that the review reflects an up-to-date understanding of the field. This helps incorporate the latest methodologies, findings, and technological advancements, which strengthens the validity of this review. The population consists of children from both industrialized and developing nations. The selected study designs were cross-sectional, longitudinal, cohort, review, and systematic review. The analysis of research entailed reading titles, abstracts, and complete texts. Following these processes, thirty articles were considered for review. The broad investigation aims to reveal the effects of body composition on aerobic fitness levels and hemodynamic parameters in preventing childhood obesity. MeSH headings related to “body composition,” “overweight,” “obesity,” “physical activity,” “heart rate,” “blood pressure,” “aerobic fitness,” “nutrition,” “cardiovascular disease,” and “children aged 10-18 years old,” were found by a keyword search and were fused and then detonated. The searches only incorporated peer-reviewed English-language articles. For discussion, categories of original articles were created. Fig. (1) displays how articles were selected.
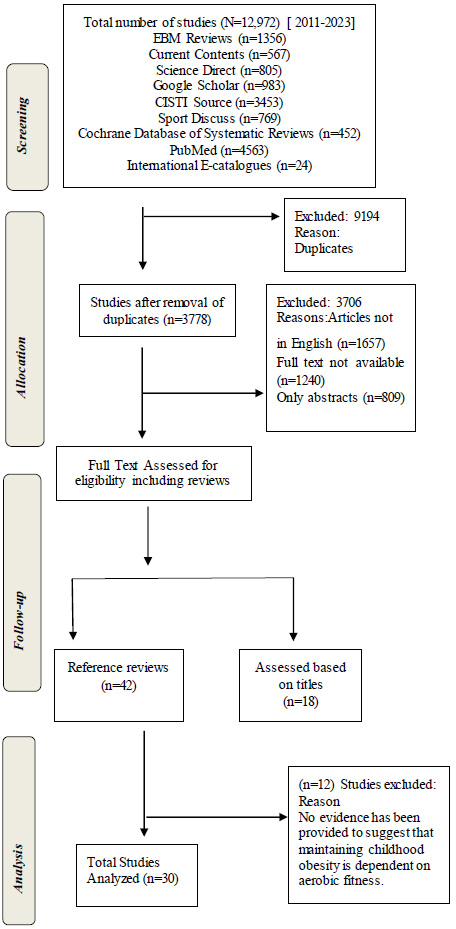
PRISMA flow chart of the study selection process.
2.2. Inclusion Criteria
The studies meeting the requirements for this review included MeSH headings such as “body composition,” “overweight,” “obesity,” “physical activity,” “heart rate,” “blood pressure,” “aerobic fitness,” “nutrition” “cardio- vascular disease,” “and “children aged 10-18 years old.” These headings were identified through a keyword search and subsequently compiled for analysis. As indicated in the data sources, articles from 2011 to 2024 were searched using all the aforementioned headings. The population consists of children from both industrialized and developing nations. The selected study designs were cross-sectional, longitudinal, cohort, review, and syste- matic review. The analysis of research entailed reading titles, abstracts, and complete texts. Following these processes, thirty articles were considered for review. The broad investigation aims to reveal the effects of body composition on aerobic fitness levels and hemodynamic parameters in preventing childhood obesity. This research will serve as a foundation for further investigations aimed at identifying factors to reduce childhood obesity and promote the importance of children engaging in aerobic fitness.
2.3. Exclusion Criteria
Several exclusion criteria were implemented to ensure the inclusion of only relevant research in this review. Specifically, only full-text papers published in English were considered for the objectives of this review. Additionally, publications were excluded if they did not focus on childhood obesity as the primary outcome. Furthermore, studies were disqualified if they did not provide evidence supporting the significance of aerobic fitness levels in preventing childhood obesity.
2.4. Data Extraction
The papers included in the study were categorized based on the journals or conferences in which they were published, along with relevant keywords, grouping them into two main themes: “obesity and aerobic fitness in children” or “importance of PA in children.” Once the data extraction process was completed, information was compiled, including details on analysis procedures, window selection, and geographical aggregation methods, to assess the contributions of each study to promoting proper levels of PA. Additionally, data regarding the correlation between obesity and aerobic fitness levels in children, the problem definition or review objective, and the presence of a theoretical explanation of strategic conduct were collected to evaluate the comprehensibility of the included research. Subsequently, all findings were organized and consolidated into a unified framework to provide a cohesive structure for analysis.
3. RESULTS
We discovered 12972 publications related to childhood obesity, hemodynamic variables, PA, and aerobic fitness; however, 9194 articles were deleted due to duplication. The number of studies left after removing duplicates was 3778. Furthermore, 1657 articles were removed because they were not in English, 1240 articles had no full text available, and 809 articles only included abstracts. Moreover, Full Text was reviewed for eligibility, which included 42 reference reviews and 18 titles. Table 1 shows the final selection of thirty articles for this review analysis.
| Author\Refs. | Journal & Year | Study Design & Sample Size | Results |
|---|---|---|---|
| Gowme et al. [10] | Journal of Primary Health Care & Family Medicine (2022) | Cross-sectional study N= 870 Age 9-14 years old |
The results of the non-parametric Spearman's rho correlation coefficients revealed several significant and negative relationships between physical fitness and body composition measurements, which were stronger in girls than in boys |
| Toriola et al [11]. | African Journal for Physical Health Education, Recreation and Dance (2012) | Longitudinal Study (PAHLS N=283 |
It was concluded that girls were more overweight and less active than boys. In view of the health implications of the findings, there is a need to create an enabling environment and opportunities that will promote a physically active lifestyle and develop life-long positive attitudes towards PA among the learners |
| Köchli et al. [12] | Frontiers in pediatrics (2012) |
Cross-sectional study N= 1,324 Aged 7.2 ± 0.4 years |
Increasing BMI was associated with higher CPP, but did not remain significant after adjustment for CRF and heart rate. |
| Bourke et al. [13] | Journal of Behavioral Nutrition and Physical Activity (2023) |
A systematic review and meta-analysis | The weight of available evidence suggests that the majority of young children are adhering to the overall recommendation and the individual TPA and MVPA aspects of the recommendation. |
| He et al. [14] | Preventive medicine (2011) |
N=1795 Age 8-13 years old |
Significantly higher CRF was found in children with normal weight (from 6.55 to 8.65ml/kg/min) or physically active children (from 0.42 to 1.22ml/kg/min) compared with the reference group. CRF was inversely associated with the kg/m2 change in BMI during the follow-up period (β=−0.63kg/m2 and −0.64kg/m2 for boys and girls, respectively, both p<0.001) |
| López-Gil et al. [15] | International journal of environmental research and public health (2011) |
N=370 Age 6-13 years old |
Children that presented normal weight achieved higher results for health-related physical fitness and physical activity than those with excess weight; this was, however, not found to be the case for sedentary behaviour. |
| Pepera et al. [16] | BMC Sports Science, Medicine and Rehabilitation (2022) |
N=105 | Children with normal BMI tend to present better CRF performance than obese and overweight children. Sedentary behaviour is associated with lower CRF in primary school-aged children. |
| Aires et al. [17] | Journal of Physical Activity and Health (2010) |
Cross-sectional study/ N=111 Age 11-18 years old |
This paper provides evidence that BMI was inversely and significantly correlated with CRF. Only CRF was correlated with vigorous and very vigorous PA levels and the total amount of PA. |
| Sayyah et al [18] | AI and Tech in Behavioral and Social Science (2024) |
Cross-sectional study N=542 |
The results showed significant differences in BMI and waist-to-hip ratios among elementary, secondary, and high school students (P<0.0001), except for the waist-to-hip ratio of high school students (P=0.699). Additionally, there was a significant association between being overweight and access to sports facilities at home for secondary and high school students (P=0.000, P=0.014), but not for elementary students (P=0.384). Based on the findings of this research, access to sports facilities at home and school significantly contributes to the health conditions of students at all school levels. Therefore, school authorities and parents should ensure sufficient sports facilities are available for children. |
| Wang et al. [19] | BMC Pediatrics (2023) |
A systematic review and meta-analysis | Physical activity can effectively improve the body weight, maximal oxygen consumption, heart rate, systolic blood pressure, and diastolic blood pressure of obese children and adolescents. |
| Hjorth et al. [20] | International Journal of obesity (2014) |
N=785 Ages 8–11 years |
In the longitudinal study design, a high-fat mass index at baseline was associated with lower PA and higher sedentary time after 200 days but not vice versa, even in normal-weight children. Our results suggest that adiposity is a better predictor of PA and sedentary behavior changes than the other way around. |
| Pinto et al. [21] | Obesity Research Open Journal (2019) |
A Systematic Review | Studies with twins and adopted children show that 55 to 80% of the variation of body mass index (BMI) is attributed to genetic factors. |
| Tsoi et al. [22] | Obesity Facts (2022) |
Age 2–19 years old | The prevalence of obesity and severe obesity increased from 14.7 [95% confidence interval: 12.9–17.0]% to 19.2 [17.2–21.0]% and 3.9 [2.9–5.0]% to 6.1 [4.8–8.0]% in 1999–2018, respectively (p = 0.001 and p = 0.014, respectively). |
| Celik et al. [23] | European Journal of ophthalmology (2022) |
N=65 | Peak systolic and end-diastolic velocities were found to be significantly lower in obese children than in controls in all three examined arteries (p < 0.05). |
| Burgos et al. [24] | Arquivos Brasileiros de Cardiologia (2013) |
N=1,950 Age 7 to 18 years. |
WC was positively correlated with BMI (r = 0.85; p < 0.001) and BP (SBP r = 0.45 and DBP = 0.37; p < 0.001) |
| Agostinis-Sobrinho et al. [25] | The Journal of Pediatrics (2018) |
A longitudinal analysis N= 734 Age 12-18 years old |
Adolescents with persistently low levels of cardiorespiratory fitness exhibited the highest levels of systolic BP and rate pressure product. |
| Brito et al. [26] | Brazilian Journal of Medical and Biological Research (2014) |
A review | Many factors may influence postexercise hypotension hemodynamics, and future studies should directly address these specific influences because different combinations may explain the observed variability in postexercise hemodynamic studies. |
| Wellman et al. [27] | The Journal of Clinical Hypertension (2020) |
A longitudinal study N= 993 Ages 12.8, 15.2, and 17.0 years |
Our findings support recommendations that adolescents engage in at least moderate PA on a regular basis to prevent the development of BP in the hypertensive range. |
| Gerber et al. [28] | International Journal of environmental research and public health (2022) |
N= 1090 Age = 8.3 ± 1.4 years). |
77.1% of the children engaged in ≥60 min of MVPA/day. Girls were more likely to be O/W and accumulate less than 60 min of MVPA/day and had significantly higher relative body fat than boys (p < 0.001). |
| Tremblay et al. [29] | International Journal of behavioral nutrition and physical activity (2011) |
A systematic review Age 5-17 years old school children |
In particular, the evidence suggests that daily TV viewing in excess of 2 hours is associated with reduced physical and psychosocial health and that lowering sedentary time leads to reductions in BMI |
| Cristi-Montero et al. [30] | Journal of sport and health science (2019) |
Cross-sectional study N= 548; boys, 47.3%; 14.7 ± 1.2 years) |
The cardiometabolic risk score was lower in adolescents meeting the MVPA recommendation and with less time spent in SB in comparison to the high-SB & Inactive group (p < 0.05). |
| Bull et al. [31] | British Journal of Sports Medicine (2020) |
N/A | These 2020 WHO guidelines update previous WHO recommendations released in 2010. They reaffirm messages that some physical activity is better than none, that more physical activity is better for optimal health outcomes, and provide a new recommendation on reducing sedentary behaviours. |
| Ruggieri & Bass [32]. | Journal of School Health (2015) |
A review | Prolonged sedentary behaviour negatively impacts children’s aerobic fitness levels and also increases the risk of obesity and CVD. |
| Vazquez &Cubbin [33]. | Current obesity reports (2020) |
A review of the literature | Evaluation of the relationship between SES and obesity in children is complicated by the complexity of SES and the lack of a common definition. |
| Mekonnen et al. [34] | Scientific reports (2021) |
Cohort Study N= 59,927 1 month to 8 years |
These results suggest that social inequalities in children’s BMI present early in infancy and continue to 8 years of age. The inequalities sometimes differed according to the indicator of socioeconomic position used. Interventions to combat these inequalities early in life are, thus, needed |
| Kambondo & Sartorius [35]. | International Journal of Environmental Research and Public Health (2018) |
Cross-sectional study N=974 |
This study has identified prominent proximal determinants of overweight/obese and overfat/obese among primary school children in Zimbabwe to better assist policy guidance. |
| Stamatakis et al. [36] | Preventive Medicine (2013) |
N=17,509 Children Age 2– 13 years old |
V viewing was positively associated with adiposity in children after adjustment for covariates. ► There was evidence of an inverse association between PC time and BMI SDS, but not the sum of skinfolds. ► Associations between screen time and adiposity differ by type of screen time and adiposity marker. |
| Chung et al. [37] | Obesity reviews (2016) |
A systematic review Age 2-18 years old children |
Since 2000, the majority of studies have demonstrated no change or a decrease in prevalence among both high and low SEP groups. However, around 40% of studies indicated a widening of socioeconomic inequalities post‐2000. While our study provides grounds for optimism, socioeconomic inequalities in overweight and obesity continue to widen |
| Drewnowski.[38 | Obesity treatment and prevention: new directions (2012) |
N/A | Higher obesity rates in poor neighborhoods may be the toxic consequence of economic insecurity. Alleviating poverty may be the best, if not the only, way to stop obesity |
| Navti et al. [39] | BMC Public Health (2014) |
Cross-sectional study N= 557 Age 5 -12 Years old |
The highest frequencies of overweight/obesity (18.8%), abdominal overweight/obesity (10.9%), and high body fat/obesity (12.3%) were observed among the tallest children from a high socioeconomic background. |
4. DISCUSSION
The purpose of this review was to examine the effects of body composition on aerobic fitness and hemodynamic variables in children and adolescents due to the rising prevalence of O/W and childhood obesity brought on by the inability of children to engage in PA and to maintain a healthy, appropriate body composition. Therefore, thirty studies were deemed eligible for this review. The impact of PA on body composition is linked to its influence on reducing the risk of obesity in children [16]. Other substantial physical health advantages of maintaining a high level of PA include favorable impacts on body composition, blood pressure, metabolic profile, muscular growth, and bone mineral density [14, 17]. Additionally, maintaining a healthy age-appropriate weight in children is greatly influenced by engaging in PA [15].
4.1. Association between Body Composition and Aerobic Fitness
A study conducted by Lopez et al. [15] revealed that children with normal weight demonstrated better outcomes in health-related physical fitness and physical activity compared to those with excess weight. Notably, these findings mirrored those of another study by Aires et al. [17], which similarly indicated a decline in aerobic fitness with increasing BMI among children. Additionally, Pepera et al. [16] identified a notable negative association between the aerobic fitness of children and BMI, showing that children with a normal BMI generally exhibit better cardiorespiratory fitness (CRF) than those who are overweight or obese. Those categorized as “normal” (BMI < 25 kg/m2) or “overweight” (BMI 25 to 29.99 kg/m2) demonstrated higher levels of aerobic fitness compared to those classified as “obese” (BMI > 30 kg/m2), aligning with the conclusions drawn by Aires et al. [17]. Given the fact that overweight children are more likely to carry excess weight into adulthood compared to their normal-weight peers, the prioritization of obesity prevention and treatment is imperative at this point. Furthermore, addressing obesity during childhood is vital as it is often more challenging to lose excess body composition in adulthood [16].
According to an expert survey, 12.03% of urban children are O/W or obese, and this number is rising by 8% per year [17]. This alarming statistic highlights the importance of promoting PA for the overall health of children. Studies have shown a negative correlation between aerobic fitness and childhood obesity, indicating that improving one's aerobic capacity can help prevent or reduce childhood obesity [18, 19]. Regular PA not only improves cardiovascular health but also helps regulate weight by burning excess calories. As such, parents, educators, and policymakers must prioritize physical education and provide opportunities for children to engage in PA regularly [20]. Therefore, by improving one's aerobic fitness through PA, we can effectively combat the prevalence of childhood obesity and promote better health outcomes for future generations [16, 20]. Considering the comprehensive analysis presented in these studies, it is evident that children with greater levels of aerobic fitness are less likely to experience obesity during their early stages of life [17, 18].
4.2. Association between Physical Activity and Childhood Obesity
The impact of PA on body composition is linked to its influence on reducing the risk of obesity in children [10, 11, 15]. Other substantial physical health advantages of maintaining a high level of PA include favorable impacts on body composition, BP, metabolic profile, muscular growth, and bone mineral density [13-22]. The American College of Sports Medicine (ACSM) recommends that children and adolescents should engage in PA. They should aim for at least 60 minutes of PA on 3-5 days per week, which can be achieved through various activities, including free play, participation in physical education, sports, using transportation, and other activities [14]. It is important to note that these activities should combine both vigorous and moderate intensity. Moderate-intensity activities are those that increase breathing, sweating, and heart rate, while vigorous-intensity activities significantly elevate breathing, sweating, and heart rate levels [14, 15].
Nevertheless, research shows that many children and adolescents still fall short of meeting the daily recommen- dation of 60 minutes of moderate-intensity PA [13, 14]. Further, it is worth noting that childhood obesity and low PA levels are associated with high obesity rates, often predicting decreased PA and increased sedentary behaviour in children [21]. Regular PA is critical for the health and well-being of children. While it primarily promotes a healthy weight, it also brings about several physical and mental health benefits [22]. As stated by Pinto et al. [21], PA has the potential to foster positive adaptations in childhood obesity and serves as a valuable tool in its prevention and treatment.
Therefore, it is important for educators and healthcare professionals to encourage children to engage in regular PA from a young age [14]. Incorporating physical education classes in schools can play a vital role in nurturing healthy habits in children [22]. Understanding the importance of PA in preventing obesity and promoting overall well-being is essential for shaping a healthier future for our children [22]. Research conducted by epidemiologists continues to emphasize that the rise in childhood obesity over the past two decades can be attributed to a variety of factors, such as inadequate PA, low levels of aerobic fitness, and excessive calorie consumption in children [3, 22]. Furthermore, PA levels have been linked to all-cause mortality, type 2 diabetes, hypercholesterolemia, hypertension, and metabolic syndrome affecting both adults and children [12, 14].
As stated by the World Health Organization (WHO), PA refers to any skeletal muscle movement that requires energy expenditure and can be performed at various intensities [14, 22]. Thus far, PA has been recommended as an effective therapeutic approach to reduce obesity-related risk factors in children and adolescents while also serving as a preventive measure against obesity in the future [19, 21]. The risk of developing obesity diminishes by 10% for every hour of moderate-to-vigorous activity in children [14]. In comparison, this review reveals that higher PA levels are associated with a reduced risk of childhood obesity [22].
4.3. Association between Hemodynamic Characteristics and Aerobic Fitness
The hemodynamic system, which includes the heart and blood vessels, plays a crucial role in maintaining aerobic fitness [23]. This intricate network of structures and processes is responsible for delivering oxygen-rich blood to all parts of the body, thus ensuring optimal functioning. The heart acts as a pump, while the blood vessels function as pathways that carry blood to and from various organs. Together, they work harmoniously to regulate BP and deliver essential nutrients throughout the body; this is especially important for maintaining aerobic fitness [22].
A well-functioning hemodynamic system is important in improving the overall health of children [22]. In light of the obesity pandemic, obesity-associated hypertension is a growing problem. A study by Burgos et al. found an association between hypertension, obesity, and cardio- respiratory fitness. Additionally, systolic and diastolic blood pressure showed significant correlations with all variables, while height, BMI, and waist circumference exhibited weak to moderate correlations [24]. However, regardless of obesity, aerobic fitness in children has been positively correlated with elevated BP levels in children with excessive body composition [23]. Moreover, children who engage in PA are less likely to have HBP, according to Agostinis-Sobesityrinho et al. [25]. Studies have indicated that regular aerobic fitness can enhance hemodynamic characteristics, such as cardiac output, stroke volume, and BP [25-27]. It works by increasing the efficiency of our heart and blood vessels, resulting in lower resting BP.
This phenomenon is known as post-exercise hypo- tension and is commonly observed after engaging in moderate to high-intensity aerobic activities. Most post-exercise hypotension cases are due to a reduction in systemic vascular resistance caused by the dilation of blood vessels during exercise [27]. This means that with regular aerobic fitness participation, children’s cardio- vascular health will improve and reduce their risk of developing hypertension or other related conditions [24]. Therefore, incorporating regular aerobic activity into children’s daily routines will help maintain their optimal hemodynamic systems and overall health [27]. Further- more, increased aerobic fitness has been demonstrated to reduce the incidence of hypertension in children and adolescents in numerous studies [24, 25]. Wellman et al. [27] found a strong correlation between HBP and prehypertension in children with low aerobic fitness levels and encouraged children to participate in at least moderate PA on a daily basis.
Overall, hypertension has become more prevalent among children and adolescents in recent years [25]. Additionally, it is well established that both children and adults can improve their aerobic fitness levels with exercise to prevent HBP [27]. Aerobic fitness, or the ability to sustain PA, relies heavily on the hemodynamic system, including the heart and blood vessels [24]. With regular aerobic exercise, this system can be improved upon. As we continue to study and understand this relationship between our bodies and PA, it is clear that prioritizing PA to improve aerobic fitness is essential for maintaining healthy well-being in children [24]. As a result, this review strongly agrees that regular participation in PA can improve hemodynamic levels in children [26, 27].
4.4. Association between Sedentary Behavior and Aerobic Fitness
Sedentary behavior is defined as sitting or lying down for extended periods throughout the day, such as watching TV or using a computer. Sedentary behaviour is becoming an increasingly prevalent issue in our society [28, 29]. Considering the rise of technology and automation, children are spending more time sitting in front of screens instead of engaging in aerobic fitness activities [29]. This has significant implications for our overall health and well-being.
Studies have shown that prolonged sedentary behavior can lead to increased risks of obesity, heart disease, and even premature death [29-31]. According to a study by Gerber et al. [28], girls were more likely to be O/W or obese and engaged in less than 60 minutes of moderate-to-vigorous physical activity (MVPA) per day. Additionally, they had significantly higher levels of relative body fat compared to boys (p < 0.001). Furthermore, children who engage in extended periods of sitting are at a higher risk of developing metabolic syndrome, which is characterized by a group of risk factors for heart disease and diabetes. This is because our bodies are designed for regular movement, and when we spend too much time sitting, our muscles become inactive, and our metabolism slows down [30]. Therefore, it is significant for children to incorporate regular aerobic activities into their daily routine to maintain good overall health and prevent childhood obesity [29, 31].
Sedentary time is a health hazard that encourages physical inactivity. Many methods of dealing with diminished PA have been recorded, all of which contribute significantly to children’s cardiorespiratory levels [29, 31]. To maintain adequate aerobic fitness levels and reduce their risk of chronic diseases, children must be cautious of their everyday activities and make conscious attempts to include more PA in their everyday lives [29, 31]. This review aligns with the findings of Ruggieri and Bass [32], who indicated that prolonged sedentary behaviour negatively impacts the aerobic fitness levels of children and also increases the risk of obesity and CVD.
4.5. Socioeconomic Status in Relation to Childhood Obesity
Childhood obesity is a growing concern, with rates on the rise in many countries [22]. To effectively address this issue, it is important to understand the relationship between socioeconomic status (SES) and childhood obesity. According to Vazquez et al. [33], weight is inversely related to socioeconomic status at given ages. This means that as children get older, their weight tends to increase, but those from lower socioeconomic status backgrounds are more likely to be obese at any given age [32]. The association between income and childhood obesity and O/W has been revealed in previous studies conducted in 2015 and 2021 [32, 33]. The aforementioned research is supported by a study by Mekonnen et al. [34], which also identified a connection between higher parental socioeconomic status and an increased risk of childhood obesity.
Furthermore, Kambondo et al. [35] discovered that high socioeconomic status was associated with a higher incidence of childhood obesity and O/W. Socioeconomic status plays a crucial role in the development of childhood obesity [36-38]. In countries that have adopted Western practices, having a low socioeconomic status is probably one of the biggest risk factors for being obese [39]. Despite an ever-widening disparity between obesity rates of low and high socioeconomic status groups, there is mounting evidence that there is a correlation between socioeconomic status and the emergence of childhood obesity [34, 38]. The prevalence of pediatric obesity has either stabilized or decreased in many wealthy nations, while it has generally increased within lower socio-economic status groups [33, 35].
This highlights the importance of considering low socioeconomic status as a risk factor for childhood obesity. As income inequality widens in our communities, particularly in nations with high rates of childhood obesity, the negative effects of low socioeconomic status are expected to worsen over time [34]. Research has consistently indicated that children from higher socio-economic backgrounds face a greater risk of obesity [36-39]. Therefore, this review supports the notion that children from lower socioeconomic backgrounds are less prone to obesity and being O/W [34, 37, 39].
5. LIMITATIONS
First, the body composition and aerobic fitness of children can vary significantly depending on their developmental stage (e.g., prepubertal vs. pubertal), making it challenging to generalize findings across age groups. Additionally, it is difficult to determine whether other factors influencing body composition may also affect CRF. The review included studies from different time periods, and the relevance of older studies may be limited due to changes in lifestyle, aerobic activity patterns, or advances in measurement techniques. Lastly, the methods used to assess CRF varied across studies, potentially leading to heterogeneity and bias in the overall effect estimates. This variability made direct comparisons between studies difficult for this review [40].
CONCLUSION
The review identifies numerous critical conclusions about risk variables related to childhood obesity prevention. One of the primary strengths of this review is its strict commitment to scientific search processes and evaluation methods. Another strength is the novelty standpoint, which examines the effects of body composition on hemodynamic variables and aerobic fitness in children [40, 41]. It emphasizes that children with normal body composition demonstrate better aerobic fitness levels compared to obese or overweight children, and higher aerobic fitness is linked with lower blood pressure values [42-44]. Additionally, reducing sedentary time is associated with increased aerobic fitness in children [45]. This review suggests the need for future research to provide clearer guidance on how to mitigate childhood obesity risks, particularly by emphasizing the importance of children engaging in aerobic fitness activities [46, 47]. It also highlights a gap in the current literature concerning the role of aerobic fitness in preventing childhood obesity. In this context, priority should be given to rural school children, with findings compared to those of urban primary school children [48]. Overall, this review concludes that the risk of childhood obesity can be reduced by limiting sedentary behavior, promoting proper nutrition, increasing physical activity, and encouraging participation in aerobic fitness activities to maintain a healthy hemodynamic system among children.
AUTHORS’ CONTRIBUTIONS
N. P. L.: The study concept and design were contributed; L. M.: Data analysis and interpretation were performed; G. J. B.: The paper was written; M. L. M.: Data Collection was performed.
LIST OF ABBREVIATIONS
| PA | = Physical Activity |
| CRF | = Cardiorespiratory |
| O/W | = Overweight |
| CVD | = Cardiovascular Diseases |
| AHA | = The American Heart Association |
| WHO | = World Health Organisation |
| SB | = Sedentary Behaviour |
| LMIC | = Low Middle Income |
| HBP | = High Blood Pressure |
| BMI | = Body Mass Index |
| ACSM | = American College of Sports Medicine |
| SES | = Socioeconomic Status |
| HR | = Heart Rate |
| BP | = Blood Pressure |
ACKNOWLEDGEMENTS
Declared none.

