All published articles of this journal are available on ScienceDirect.

Twelve Weeks of High-Intense Interval Training Enhance the Neuromuscular and Cardiorespiratory Performance of Elderly
Authors Info & Affiliations
Abstract
Background:
Exercise is an effective non-pharmacological intervention for the enhancement of neuromuscular and cardiorespiratory health. In particular, High-Intense Intermittent Training (HIIT) has been implicated in health management; however, in specific populations such as the elderly, is needed more investigations.
Objective:
The aim is to determine the impact of HIIT in the neuromuscular and cardiorespiratory fitness of the elderly.
Methods:
Thirty-two elderly volunteers, 71.0 ± 2.1 years, were randomly divided into two groups, control (CG) (n = 16), that did not participate in any interventions, and experimental (EG) (n = 16) that participated in a 12-week exercise program based on HIIT 3 times a week, and 40 minutes by a meeting. Both groups were subjected before and after the intervention period to neuromuscular and cardiorespiratory testing, and monthly were clinically evaluated by a Physician.
Results:
No orthopaedic events were reported to both groups, and the CG showed no enhancement to all variables. The EG, muscular endurance of the upper limbs was enhanced (p <0.0001), as was muscular endurance of the lower limbs (p <0.0001), localized muscular endurance of abdominal muscles (p <0.0001), lower limb muscle power (p <0.0001) and aerobic power (p <0.0001). There were no adverse events during or after the intervention period.
Conclusion:
HIIT is an effective strategy to promote enhancement of neuromuscular and cardiorespiratory fitness in the elderly and showed safe because no orthopaedic and cardiovascular events were reported.
1. INTRODUCTION
Previous scientific pieces of evidence have implicated the exercise with physiological changes, as well as changes in morphology and several other molecular, cellular, tissue and metabolic functions in humans. Nevertheless, several factors may affect the adaptations caused by exercise, including its volume, intensity, frequency, and type of approach [1-5]. In this context, high-intensity intermittent training (HIIT) is defined as high-intensity exercises with high-intensity stimulation in a very short duration, intermittent by recovery moments [6], which may vary according to intensity, duration, recovery period and number of intervals, among other possible variations [3].
There is evidence that this exercise approach, i.e., one with an intense and intermittent nature, stimulates physiological parameters as much as the continuous exercise of moderate-intensity does [7]. In fact, studies have shown that it may be superior in some aspects [1, 2, 8], a fact that inspires more research on the elderly subject in regards to their safety and efficacy.
Different soft tissues are acutely, subacutely, and chronically affected by exercise, and muscular tissue can be profoundly affected by exercise, not only in their morphological properties but first in physiological and functional parameters. The muscular performance stood evident in previous works; moreover, muscular dysfunctions and low performance were associated with impairment in health such as dyslipidemias, hepatic steatosis, cardiovascular diseases, bone density, brain health and cognitive performance [9-13], thus demonstrating the importance of exercise interventions to the human health, what, in fact, display the importance of this investigation, especially in elderly subjects.
Furthermore, continuous and moderate long term exercises promote increased cardiovascular capacity [8, 14], muscular hypertrophy [15], bone density [16], and have been described as a viable alternative to traditional continuous and long-lasting training. Although high-intensity intermittent training displayed strong effectiveness to develop the muscular, metabolic, and body composition enhancement, but is not useful to adolescents, people with chronic disease, or to old adults. Therefore, the objective of this study was to determine the impact of HIIT in the neuromuscular and cardiorespiratory fitness of the elderly.
2. METHODS
2.1. Ethics and Participants
Thirty-two elderly volunteers, of both genders, completed the study. No participants participated in sports or physical training on a regular basis prior to the interventions. No participants showed lesions or disease-associated conditions prior to the study. All signed informed consent forms in agreement with the Brazilian Ethics Committee that had been approved by the National Health Council under the number of CAAE 44907715.2.0000.5653 on 27/07/2015 and followed all ethical and legal requirements. We followed all conventions of the Helsinki Declaration. Baseline volunteer characteristics are displayed in Table 1.
2.2. Anthropometric Characterization
Body weights and heights were obtained using a mechanical scale (Filizolla, Brazil) with a precision of 0.1 kg. On the day of collection, the subjects were instructed to wear light clothing and to repeat the same clothing at all times of evaluation. They were placed on top of the scale barefoot, with their arms at their sides, with their eyes fixed on the horizon and standing still until the measurements could be confirmed as previously described protocols [10, 17–19]. All measurements were performed in the morning.
 |
(1) |
BMI Equation.
2.3. Study Design and Procedures
Four clinical consultations were performed with the Physician who attended to the patients, maintaining their monthly routines. These consultations occurred immediately before the intervention period, 4th, 8th, and at the end of twelve weeks of intervention. In these consultations, routine monthly clinical investigations were performed, including blood pressure, heart rate, cardiac auscultation, complete history, orthopedic investigations and other medical investigations. These procedures were performed by the same Physician.
| Volunteer Characteristics | |||
|---|---|---|---|
| Variables | CG | EG | P value |
| Age (Year) | 71.4 ± 2.48 | 70.6 ± 1.72 | 0.188 |
| Weight (Kg) | 67.3 ± 3.87 | 66.6 ± 3.08 | 0.091 |
| Height (cm) | 1.74 ± 0.6 | 1.72 ± 0.1 | 0.097 |
| BMI (Kg/m2) | 23.5 ± 0.9 | 22.5 ± 1.7 | 0.089 |
| VO2 Max (ml/kg/min) | 23.68 ± 1.54 | 24.01 ± 1.39 | 0.191 |
These consultations served as support for the control of health conditions and for reporting adverse clinical events that might be related to the intervention. Clinical, orthopedic and cardiological investigations were performed to determine possible malignant events during and after the intervention period. All consultations were performed in a blind scheme where the Physician does not know who performed or not the exercise to avoid tendencies of the outcomes in the clinical exam.
2.4. Neuromuscular Performance Assessment
All tests of this section were selected due to three aspects. First security to the application to elderly subjects, second, the convenience, facility and reproducibility and their application, and three, because all these tests showed an adequate precision and confidence, which were displayed in different previous manuscripts [ 20–23].
In order to evaluate muscular endurance, three tests were performed: one for upper limbs, one for the abdomen and one for lower limbs. The test directed for the upper limbs was arm extension with floor support (Push-Ups). The volunteer was placed in a prone position, with his or her hands resting on the ground, with a distance of 10 to 20 cm from the shoulder line, with the toes facing forward. The positioning of the hands on the ground was not above the shoulder line and, in the initial position of the movement, the subject’s face allowed for an adequate alignment between the trunk and the legs. The application of the test to females was modified only by the support of their knees on the ground. The other procedures were performed for both genders. In order to determine performance, the maximum number of correct repetitions in one minute was recorded [ 21 ].
Regarding abdominal resistance, after placing the subject in a supine position on the ground, the following exercise was performed: flexion of the trunk, hip and knees, embracing the legs with the arms; in order to determine performance, the maximum number of repetitions in one minute was recorded [ 22,23].
The execution of the jump, an eccentric phase, was carried out before it began. After the jump, the subject was instructed to remain with his or her foot at the drop site upon landing. The distance from the most posterior point of the heel to the first marking was measured with the millimeter measuring tape and considered to be the distance obtained in the jump. The jumps were performed three times and the best jump with each limb was used for statistical purposes in a horizontal flat surface [ 20 ]. They could use their upper limbs (MMSS) to aid the effort.
To determine resistance of the lower limbs, an isometric test was selected. The subjects were placed with their backs supported on the wall. Isometric hip, knee and ankle flexion were performed at 90º with the aid of a goniometer. The time was recorded for performance effect. Subjects who were able to maintain this position for longer than one minute performed the test with only one lower limb after a 10-minute recovery period; during this second test, the extra limb was crossed on top of the limb that was resting on the ground, and soon thereafter the subject switched sides [ 20 ].
2.5. Cardiorespiratory Fitness Assessment
To determine their respiratory capacity, the 6-minute walk test (TC6M) was performed outdoors. The subjects walked at their own pace and alone, as far as possible during the six minutes; knowing the possible cardiorespiratory changes that might arise, they were allowed to walk slowly, stop, relax when necessary, and begin walking again when they felt ready to resume the exercise. Each individual was encouraged to wear light clothing and not to exercise prior to the test. The following equations determine the level of walking distance predicted for each test performed on the patient:
Men:
Distance TC6M (m) = (7.57 x height cm) - (5.02 x age) - (1.76 x weight Kg) – 309 m
Women:
Distance TC6M (m) = (2.11 x height cm) - (2.29 x weight kg) - (5.78 x age) + 667.6
Equation 1: Equation used to calculate maximum VO2.
It should be emphasized that the anthropometric and performance evaluations were only performed 60 days after the beginning of the intervention, because the literature is categorical in stating that 30 days are insufficient for anthropometric and performance measurements to have changed enough to show differences, even in sedentary people.
2.6. Training Protocol
A high-intensity interval training program was applied three days a week, with an average duration of 40 minutes per meeting. All exercises were performed without equipment, using the subject’s body weight alone. Each exercise set was done against the clock at a ratio of 1:2, between activity and rest. The exercise intensity was set up at a minimum of 80%, or more, during the stimuli and twice the time to passive recovery to cardiac frequency decrease. During the recovery, the heart rate reached low levels of about 55% of the max cardiac rate. The control of the cardiac frequency was performed by utilization of the FTI model Polar heart monitor with an observation of the heart frequency immediately after the stop of the challenge for all subjects.
Daily, a standardized 5-minute warm-up with stretching exercises and calisthenics was performed for 5 minutes. Subsequently, the main work out was performed, consisting of forward-backward running, squats, push-ups, sit-ups, jumping jacks, walking lunges, dips, six-point support planks, pulse lunges, reverse lunges, skipping, mountain climbers, arm and leg raises, side steps, direction-changing footwork and climbing/descending steps (25 cm).
Finally, a 5-minute cooldown was carried out to promote calmness. Each exercise was performed for 30, 45 or 60 seconds for recovery, always 2x greater than the stimulus time. In addition, all classes had approximately 10 minutes of stimulation. During all the moments of rest between one stimulus and another, the subject was free, yet encouraged to remain quietly awaiting the next stimulus in order to characterize a passive rest.
2.7. Statistical Analysis
The descriptive data were expressed as mean ± standard deviation. To determine the normality of the data, the Shapiro–Wilks test was performed, which determinate that the data are non-parametric type. Then, the Kruskal–Wallis with Dunn’s posterior test was used to determine the difference between the days of experiments. Additionally, the effect size was calculated by Choen’s D test, indicating that when the calculated differences (d 2 ) are between 0.01 and 0.14, the effect is defined as little, from 0.15 to 0.34 defined as a medium effect, and 0.35 more, the effect was considered large. All hypothesis tests had a significance of 5%. The entire statistical procedure was performed using the Prism Stat 5.0 program.
3. RESULTS
3.1. Clinical Investigations Reported No Orthopedic and Cardiac Events
Four clinical consultations were performed with the Physician immediately before the intervention period, four, eight, and at the end of the intervention to serve as support for the control of health conditions and for reporting orthopedic and cardiological adverse clinical events. All investigations in all data points showed no events reported.
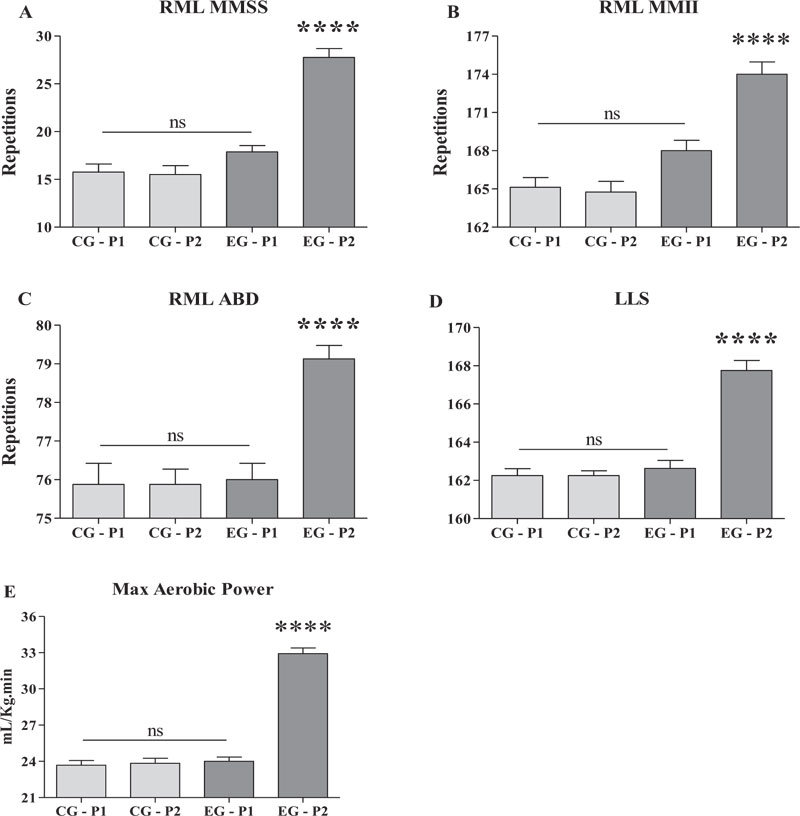
3.2. HIIT Improves the Physical Capacity of the Elderly
With respect to the localized muscular endurance of the upper limbs (Fig. 1A), for the CG at baseline (P1), the value was 15.75 ± 2.43 and at P2, the value was 15.5 ± 2.67 (p >0.05). For the EG at P1, the value was 17.88 ± 1.88 and at P2, it was 27.75 ± 2.65 (p <0.0001) for all comparisons. Cohen’s d showed a medium-size effect (d2= 0.33).
With respect to the localized muscular endurance of the lower limbs (Fig. 1B), for the CG at baseline (P1), the value was 165.1 ± 2.16 and at P2, it was 164.8 ± 2.37 (p >0.05). For the EG at P1, the value was 168 ± 2.33 and at P2, it was 174 ± 2.72 (p <0.0001) for all comparisons. Cohen’s d showed a medium-size effect (d2= 0.32).
With respect to the localized muscular endurance of the abdominal muscle (Fig. 1C), for the CG at baseline (P1), the value was 75.88 ± 1.55 and at P2, it was 75.87 ± 1.12 (p> 0.05). For the EG at P1, the value was 76 ± 1.19 and at P2, it was 79.13 ± 0.99 (p <0.0001) for all comparisons. The Cohen’s d showed medium-size effect (d2= 0.27)
In terms of lower limb muscle power (Fig. 1D), for the CG at baseline (P1), the value was 162.3 ± 1.03 and at P2, it was 162.3 ± 0.7 (p >0.05). For the EG at P1, the value was 162.6 ± 1.18 and at P2, it was 167.8 ± 1.44 (p <0.0001) for all comparisons. The Cohen’s d showed medium-size effect (d2= 0.29)
In terms of aerobic power (Fig. 1E), for the CG at baseline (P1), the value was 23.68 ± 1.54 and at P2, it was 23.85 ± 1.61 mL/Kg/min (p >0.05). For the EG at P1, the value was 24.01 ± 1.39, and at P2, it was 32.91 ± 1.91 mL/Kg/min (p <0.0001) for all comparisons. The Cohen’s d showed large size effect (d2= 0.53)
4. DISCUSSION
The literature demonstrates positive evidence between the practice of exercise and sports and the health benefits of different populations [9, 24]. Within this context, it has been shown that intermittent and high-intensity exercise has important effects on adult health [2, 25]; furthermore, it improves physical performance [26] in a manner similar to that obtained from continuous exercise.
The present study aimed to investigate the effects of high-intensity intermittent training (HIIT) on health, body composition and physical performance of elderly individuals, findings not yet explored in the literature, because most of the studies have been done with healthy young adults [3]. For physical performance, cardiovascular fitness and evidence of clinical, we recorded orthopedic and cardiovascular results.
We found that high-intensity intermittent training can be a safe and effective strategy for the modification of factors related to cardiorespiratory health. To the best of our knowledge, there had been no reports of cardiovascular, orthopaedic, and/or another clinical depreciative event. These facts provided pieces of evidence for the safety of this approach in older adults even when, during the intervention, the stimuli surpassed 80% of the maximum heart rate, showing a high level of intensity as HIIT suggests. It is important to mention that the control group (CG) showed no modifications from the P1 to P2; therefore, the discussion will focus on explaining results in the experimental group (EG).
There has been evidence to suggest that various types of physical exercises and ways of applying training programs modify neuromuscular factors. In a study carried out with athletes who practice Pilates, after 60 days of training with similar characteristics in terms of having interval characteristics, but with lower intensity, the method was able to modify flexibility, RML MMSS and ABD; nevertheless, it was not able to modify body composition [10]. These data are important because they demonstrate that the intensity of the training can have a determining effect on the measurements of physical performance, as both moderate and intense exercises applied intermittently were able to modify the parameters studied here, corroborating the results found here, by exhibiting different modifications. Our data corroborate, in part, the current literature on the subject [17, 27].
By contrast, continuous and long-term exercises may or may not also affect the body composition of healthy adults; including visceral fat that has been strongly related to increased risk for the development of cardiovascular diseases and cerebrovascular accidents [27, 28], corroborating what has been demonstrated here.
One difficulty of the present study, however, is related to finding studies that used HIIT in the elderly population . We might suggest that the present study is one of the first, investigating the effects of HIIT in this population. Previously, we conducted a pilot study in this population (n = 4) and in adults close to senility (n = 4), however for a period of 180 days (unpublished data). This pilot previously demonstrated the safety and efficacy of HIIT in this population, and encouraged us to expand the sample, and perform a new study with similar characteristics in this population that is most vulnerable to cardiovascular and metabolic diseases.
A number of recent studies with interval training studies have demonstrated the efficacy of intermittent and high-intensity exercise on human health and performance [1, 2, 8, 29]. It has been demonstrated that HIIT can improve cardiovascular conditioning, a factor that is fundamentally related to the reduction of the risk of myocardial, neural or peripheral vascular diseases and accidents [30]. It is, therefore, one of the most valuable findings of the present study. Combined with the modification of blood lipid profiles and muscle performance that had been reported in the present study, it can be safely stated that HIIT promotes improvements in metabolism and the cardiorespiratory system.
These results are even more relevant because high-intensity interval training, on account of its intense nature, has not been thoroughly investigated in the elderly population; nevertheless, it was evident here that the training application did not cause cardiovascular or orthopedic damage. In fact, we found that this modality preserves bone, muscle and joint integrity in this population that did not have any diseases or injuries previously identified in their medical appointments and in the physical evaluations performed.
The investigated population differs fundamentally in age from those of other scientific investigations, making the application of a methodology of high-intensity exercises problematic, primarily because of the scarcity of data in the literature. Nevertheless, despite the fact that the entire program was inspired by a study carried out with young adults [2, 8], none of the subjects reported any orthopedic complications or any type of vascular accident, suggesting that it appears to be safe.
Analyzing the efficacy of the HIIT, even without another method to perform a comparison, which is a limiting factor for the present investigation, the size effect was never displayed less than medium, and, to the cardiorespiratory fitness, the size effect was large. This data showed that HIIT could be a good choice to develop the physical performance of the neuromuscular and cardiorespiratory systems of the elderly. This notion, together with the fact that this study takes lightly the safety of this approach, allows affirming that the HIIT is a valorous tool in the context of the physical exercise and health.
Although the data discussed here suggest HIIT is safe in an elderly population, a recent review would suggest that HIIT may induce a greater number of cardiovascular events than continuous moderate-intensity exercises when applied to people with the coronary or arterial disease [31, 32]. Therefore, although the volunteer population of this study was healthy, it is recommended that health conditions be carefully evaluated before applying HIIT [33-35].
CONCLUSION
There was a significant improvement in muscular and cardiorespiratory performance. Likewise, there was no evidence of health impairment in volunteers and no adverse events after sixty days of intermittent high-intensity training, suggesting that this training modality is effective as a tool for the prevention of cardiovascular and metabolic diseases as well as to improve various factors related to the health of the elderly.
We recommend that this approach should be observed for a longer period of time with longer longitudinal interventions in order to assess the safety and efficacy of long-term HIIT for this particular population and to evaluate the effects of different daily and weekly doses in order to obtain ideal benefits to human health.
AUTHORSHIP CONTRIBUTIONS
All authors contributed equally to study design, writing, data treatment and final text approval. JRVS and FEFL performed the data collection.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study is approved by the Brazilian Ethics Committee of the National Health Council under the number of CAAE 44907715.2.0000.5653 on 27/07/2015 and followed all ethical and legal requirements.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures were followed in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Written informed consent was obtained from all participants.
AVAILABILITY OF DATA AND MATERIALS
Not applicable.
FUNDING
None.
CONFLICT OF INTEREST
The author declares no conflict of interest, financial or otherwise .
ACKNOWLEDGEMENTS
Declared none.

