All published articles of this journal are available on ScienceDirect.

Prevalence and Risk Factors of Ankle Sprain Among Male Soccer Players in Tabuk, Saudi Arabia: A Cross-Sectional Study
Abstract
Background:
Ankle sprains are common among soccer players, and their risk factors are well documented in the literature. In Saudi Arabia, some healthcare and sport-related characteristics provide the necessity for investigating the prevalence and risk factors of ankle sprain in that region as well.
Objective:
To analyze the prevalence of lower limb injuries and risk factors of ankle sprains among male soccer players in Tabuk, Saudi Arabia.
Methods:
A cross-sectional study among 400 male soccer players from different sports clubs in Tabuk, Saudi Arabia was conducted. A self-structured questionnaire was used to collect data related to ankle sprains. Chi-square, Fisher’s exact tests, and unpaired t-tests were used to test the association between variables. Univariate logistic regression analysis was used to identify the risk factors.
Results:
Ankle sprains were the most prevalent, reported by 63.8%. Previous ankle injury, lack of stretching, lack of warm-up, and not wearing bracing were identified as significant risk factors. A total of 47.9% of players preferred to go to the hospital for treatment, 15.8% selected physical therapy, while 56% had no prior education regarding injury prevention.
Conclusion:
Ankle sprain is the most prevalent lower limb injury. Risk factors include previous ankle injuries, lack of stretching, lack of warm-up, and not wearing bracing. Players have little knowledge of physical therapy measures and lack of injury prevention education. Our findings suggest that increasing the awareness of injuries and proper physical therapy measures might assist in preventing recurrence of ankle sprains among male soccer players.
1. INTRODUCTION
Soccer (or football) is the most popular sport in Saudi Arabia [1]. Ankle sprain is the most common lower limb injury experienced by individuals involved in physical activity, comprising approximately 80% of ankle injuries [2, 3]. Ankle sprain injuries usually occur during landing on irregular surfaces, such as the foot of another player, or incorrect foot positioning at landing, resulting from delayed reaction time of the peroneal muscles or a tackle from the medial side [4, 5]. Recurrent ankle sprains account for approximately 16% of all ankle sprains [6]. Studies have reported that the ankle reinjury rate in soccer is between 4% and 29% [7-9]. One recent study from Saudi Arabia reported ankle injuries (n = 399) in physical education and sports among Saudi high school male students in Riyadh. The authors found that the range of prevalence of ankle injuries was 14%-34.7% [10].
Several studies found that soccer injury rates varied depending on competition level, age, and gender [11-13]. During the 2010 FIFA World Cup competition, ankle sprain was the most prevalent condition, and approximately 50% of players were prevented from participating in the competition [14]. The recognition of risk factors leading to ankle sprain appears to be the keystone for effective ankle sprain injury prevention strategies [15]. Two types of risk factors are suggested: extrinsic and intrinsic risk factors. Extrinsic risk factors include the total amount of training and number of played games, climatic factors, pitch surface, playing field status, equipment, and rough play. Intrinsic risk factors include joint flexibility, instability, preceding injuries, and inadequate rehabilitation [16-18].
Previous studies reported that players with histories of ankle sprain, players wearing air-filled heel shoes, and players who did not stretch the ankle joint structure before exercising were 4.9, 4.3, and 2.6 times more likely to withstand an ankle sprain [19]. Limited dorsiflexion movement in the ankle [20], the usage of artificial turf ground while playing soccer [21], and posteriorly-positioned fibula [22] were also reported as risk factors for ankle sprains.
Previous ankle injury is one of the most common risk factors for acute ankle injuries; therefore, it is very important to recognize strategies for preventing first-time occurrence of acute ankle injuries [23, 24]. In order to prevent acute ankle injuries, some players use ankle braces during sports activities. A few systematic reviews reported that ankle bracing was effective in reducing the re-occurrence of ankle sprain among athletes [25, 26]. The benefits of taping, neuromuscular exercising, and bracing for preventing injuries during team sports have been emphasized in the literature [27, 28]. Appropriate warm-up and stretching exercises are the most commonly recommended measures for the prevention of acute sports injuries [29, 30]. A few studies suggested performing warm-up exercises prior to sports activity to reduce the risk of injury [31-33].
Based on the theoretical framework for injury prevention, effective actions should be directed towards the adjustment of the player’s attitude and behaviors regarding risk factors and prophylactic measures [34, 35]. Because of the rate of recurrence and debilitating nature of these injuries, it is critical for coaches or trainers, physical therapists, and physicians to identify leading risk factors for ankle injury. This would assist in the application of preventive measures and, in turn, would reduce the likelihood of injury occurrence and recurrence.
Tabuk region is located in the northwest part of Saudi Arabia. The Jordanian border bounds it from the north and the red sea from the west. It is known by its colder climate in comparison to other regions of Saudi Arabia. In terms of sport, Tabuk has four professional soccer clubs and one stadium that hosts local soccer competitions. There are also a number of public and private soccer fields, turfed and non-turfed, scattered all over the region. Presently, sport-related healthcare professionals are relatively less in number in the Tabuk region, and there are no specialized clinics or hospitals for athletic or sports injuries. The only available options of treatment in Tabuk for injured athletes are general medical facilities. All these healthcare and sport-related factors provide the necessity for investigating the prevalence and risk factors of ankle sprain in Tabuk region, and how these data may differ from what was reported in the literature. To date, there are insufficient studies of ankle sprain injuries among soccer players in Tabuk and other regions in Saudi Arabia. In this study, therefore, we analyzed the prevalence of lower limb injuries and risk factors of ankle sprain among male soccer players in Tabuk, Saudi Arabia. It was hypothesized that, in male soccer players, there will be a high prevalence rate of ankle sprain among the lower limb injuries. We also hypothesized that there will be significant demographic and play-related risk factors correlated with ankle sprain rates.
2. MATERIALS AND METHODS
2.1. Participants
This cross-sectional study was conducted from February to August 2018. A total of 400 male soccer players, professionals and amateurs, from four sport clubs in Tabuk, Saudi Arabia were recruited using a convenience sampling method. This sampling method was utilized due to the limited number of sports clubs and difficulties to access the soccer players at any time. The sample size was determined using the prevalence and risk factors of ankle sprain among the soccer players in the study population. This was calculated using a power of 80% and α = 0.05 to detect a difference of 20%. Accordingly, a total sample size of at least 400 was determined. The inclusion criteria were as follows: current soccer players (professional or amateur); between 18 and 40 years of age; and male gender (because this game is uncommon among females in Saudi Arabia). The exclusion criteria were as follows: any underlying inflammatory symptoms (e.g., redness, swelling, pain, limited range of motion) assessed through taking a full history, and any ankle or foot congenital diseases or abnormalities.
2.2. Questionnaire
A self-structured questionnaire that was based on previous research [15] was used in this study. The questionnaire collects data relating to (1) basic demographics such as age, marital status, educational level, height, weight and body mass index (BMI); (2) occurrence and recurrence of ankle sprain among other lower extremity regions; and (3) potential risk factors, including play field-related characteristics, play environment, recurrence of injury, previous ankle injury and type of management taken, knowledge of physical therapy, received physical therapy treatment and education. The questionnaire is distributed among the participants and collected by the researchers on the same day, with the researchers presented all the time to answer any questions regarding the questionnaire. The items of the questionnaire were presented in a language appropriate for players. It was pilot-tested in a group of 10 players. The players faced no major difficulties and they could understand the questions and the response options.
2.3. Data Analysis
All categorical data are expressed as the frequency with percentage; continuous data are expressed as mean with standard deviation. Significance and associations between the dependent and independent variables were tested using Chi-square tests, Fisher’s exact tests, and unpaired t-tests. All significant variables from the Chi-square analysis were tested further using a univariate logistic regression model. The goodness of fit of the univariate logistic regression model was 0.789. All analyses were performed using SPSS 21.0 version. p-values less than 0.05 were considered significant.
3. RESULTS
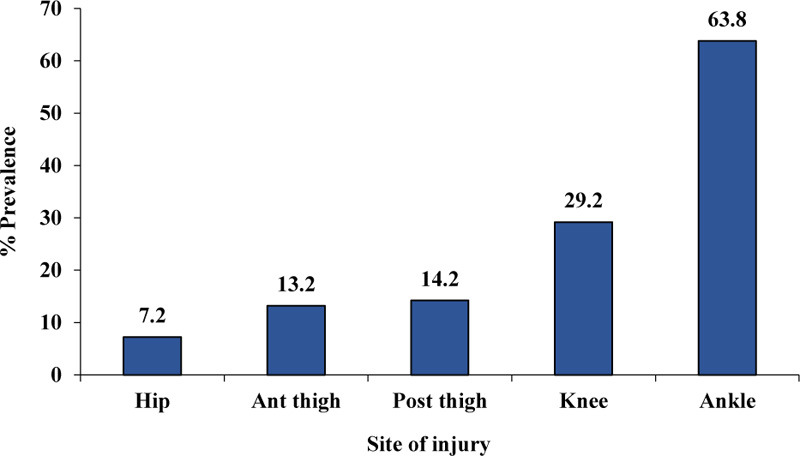
A total of 400 participants with a mean age of 23.2 ± 5.9 years participated in the study. The characteristics of the participants are shown in Table 1. As illustrated in Fig. (1), ankle injury (63.8%) represented the highest percentage of complaints among all lower limb injuries. A total of 47% of the players reported injury of the right ankle, 24% of the left, and 29% in both. For those with ankle sprains in the previous year, about 42% suffered the sprain more than once, while the rest had it only one time. None of the demographic variables (age, BMI, duration of playing soccer, etc.) were significantly associated with the frequency of ankle sprain (one and more than one time) on Chi-square or Fisher exact or unpaired t-test (Table 2). The Chi-square or Fisher exact test and univariate logistic regression analysis revealed that previous ankle injury, lack of stretching, lack of warm-up and not wearing bracing were significant risk factors for ankle sprain incidence regardless of injury frequency (Tables 3 and 4). The remaining risk factors were not found to be significant (Tables 3 and 4). Of those with ankle sprains, 47.9% preferred to go to the hospital for treatment, while 33.2%, 15.8% and 3.1% chose to rest, undergo physical therapy, and other treatments, respectively. A total of 56% of players had no prior educational background regarding injury prevention.
4. DISCUSSION
This study was conducted to evaluate the prevalence and risk factors of ankle sprain among male soccer players in the Tabuk region, Saudi Arabia. We hypothesized that there will be a high prevalence rate of ankle sprain among the lower limb injuries. We also hypothesized that there will be significant demographic and play-related risk factors correlated with ankle sprain rates. The results of this study partially support our proposed hypotheses in that ankle sprain was the most prevalent, reported by 255 of 400 participants (63.8%), with 58% and 42% reporting ankle sprain once and more than once within the prior 12 months, respectively. Some risk factors were found to be significant in our study, including previous ankle injury, lack of stretching, lack of warm-up, and not wearing bracing. However, none of the examined demographic factors was found to be significantly correlated with ankle sprain incidences.
Several authors found previous ankle injury as a significant risk factor for the recurrent ankle sprain. One group reported that 60% of the ankle sprains occurred in players with a history of previous ankle sprains [4]. In another study, 9 of 13 ankle sprains (69%) were associated with a history of previous ankle sprains [36]. Soccer players having a previous history of ankle sprain injury were 4.9 times more likely to sustain a recurrent ankle sprain injury than players without previous ankle sprain injury [5]. Tropp et al. [37] also reported that players with a history of ankle injury are at a higher risk of future injury than players with no previous injury. These findings are consistent with those of the present study.
Most of the players acknowledged using regular stretching exercises for injury prevention; stretching exercises are commonly used for warm-up or cool-down routines [38] and are useful to increase muscle extensibility [39-41] and for prevention of sport-related injuries. Kaini et al. [42] reported that sports-specific warm-up, including dynamic stretching, could prevent injuries. In another study, it was reported that stretching exercises of certain muscles and joints for certain activities may enhance the effectiveness of these pre-exercise activities [43]. The results of these studies are consistent with those of the present study in that players who perform stretching exercises before playing have a lower risk of ankle sprain.
Warm-up exercises play an important role in the prevention of ankle sprains and their effects are well known. Warm-up is one of the most commonly suggested countermeasures for sports injury [29]. Warm-up, together with stretching exercises, enhances the flexibility of the lower extremity joints, including the ankle [44, 45]. The combination of warm-up, strength, and balance training with stretching had significant effects on the prevention of knee and ankle injuries [46-48]. These findings are strongly supportive of our results to the effect that a greater number of players developed ankle injury because of the poor performance of warm-up exercises.
In our study, we observed that not wearing bracing was a significant risk factor for ankle sprain. Ankle braces have been commonly used in sports to manage and prevent ankle sprains. One study reported a 69% reduction in ankle sprains in previously-injured athletes by using ankle braces [26]. Studies reported the use of ankle braces for the prevention of ankle sprains among active and healthy subjects [49-51]. Rovere et al. [52] reported that ankle stabilizers were effective in decreasing the occurrence of ankle injuries and that they must be worn whenever exposure to the risk of ankle injury is present. However, it is not advisable to play with a previous unhealed injury under the assumption that tapes and bandages will have a strong preventive effect [27]. This study’s results acknowledge that the use of ankle bracing reduces the incidence of ankle sprain injuries, as well as the incidence of ankle sprain injury recurrences.
We also investigated post-injury treatment measures chosen by the players. Almost half of them preferred to go to the hospital, possibly because of the severity of the injury. On the other hand, only 15.8% selected physical therapy treatment. The explanation involved a lack of physical therapy experts available in the sports field in Saudi Arabia, mainly in the Tabuk region, as well as lack of physical therapy awareness among the soccer players. Furthermore, Saudi Arabia’s healthcare system prevents patients from direct access to physical therapy services, also contributing to this finding. Analysis of injury prevention strategies among the players showed that more than half of them had never received education regarding injury prevention. Increased awareness of the mechanisms of ankle injury among soccer players, in addition to more frequent instruction and education about injury avoidance and prevention, should be addressed by trainers and team physicians. This may play an important role in reducing the incidence rate of ankle sprains in soccer players.
| Age, mean ± SD (y) | 23.2 ± 5.9 |
| BMI, mean ± SD (kg/m2) | 23.1 ± 4.2 |
| Marital Status | |
| Single Married |
332 (83.0) 68 (17.0) |
| Education level | |
| PhD Master Bachelor Diploma School |
1 (0.2) 9 (2.2) 165 (41.3) 67 (16.8) 158 (39.5) |
| Duration of playing football (y) | |
| 1-5 5-10 >10 |
37 (14.5) 88 (34.5) 130 (51.0) |
| Frequency of playing per week | |
| 1 time 2 times More than 2 times |
44 (17.3) 98 (38.4) 113 (44.3) |
| Professional football player | 87 (33.6) |
| Risk Factors | Frequency of Ankle Sprain | ||
|---|---|---|---|
|
1 time (n = 148) |
More than 1 Time (n = 107) |
P value | |
| Age, mean ± SD (y) | 23.5 ± 5.4 | 23.2 ± 6.1 | 0.689 |
| BMI, mean ± SD | 23.0 ± 4.3 | 22.8 ± 4.2 | 0.767 |
|
Marital Status, n (%) Single Married |
119 (80.4) 29 (19.6) |
93 (86.9) 14 (13.1) |
0.171 |
|
Education level PhD Master Bachelor Diploma School |
4 (2.7) 4 (2.7) 56 (37.8) 26 (17.6) 58 (39.2) |
1 (0.9) 2 (1.9) 51 (47.7) 14 (13.1) 39 (36.4) |
0.235 |
|
Duration of playing football (y) 1-5 5-10 >10 |
28 (18.9) 47 (31.7) 73 (49.4) |
12 (11.2) 39 (36.4) 56 (52.3) |
0.239 |
|
Frequency of playing per week 1 time 2 times More than 2 times |
31 (20.9) 52 (35.2) 65 (43.9) |
14 (13.1) 43 (40.2) 50 (46.7) |
0.316 |
| Professional football player (Yes) | 49 (33.1) | 36 (33.6) | 0.258 |
| Risk Factors | Frequency of Ankle Sprain | ||
|---|---|---|---|
|
1 time (n = 148) |
More than 1 time (n = 107) |
P value | |
| Type of playground Turf Non-turf |
100 (67.6) 48 (32.4) |
81 (75.7) 26 (24.3) |
0.225 |
| Footwear while play (No) | 18 (12.2) | 12 (11.2) | 0.817 |
| Previous ankle injury (Yes) | 32 (21.6) | 18 (16.8) | 0.003* |
| Surgery (Yes) | 30 (20.3) | 14 (13.1) | 0.119 |
| Functional activity (No) | 85 (57.4) | 66 (61.7) | 0.216 |
| Warm up (No) | 80 (54.1) | 51 (47.7) | 0.023* |
| Stretching (No) | 28 (18.9) | 33 (30.8) | 0.034* |
| Strengthening (No) | 115 (77.7) | 86 (80.4) | 0.680 |
| Bracing (No) | 123 (83.1) | 101 (94.4) | 0.017* |
| Taping (No) | 134 (90.5) | 99 (92.5) | 0.440 |
| Shoe-in-soles (No) | 141 (95.3) | 107 (100) | 0.669 |
*Significant at p < 0.05 level
| Risk Factor | B | P-value | OR | 95% CI | |
|---|---|---|---|---|---|
| Previous ankle injury | Yes | 1.128 | 0.042* | 1.230 | 0.454 to 2.033 |
| No | Reference group | - | - | - | |
| Stretching | Yes | Reference group | - | - | - |
| No | 0.778 | 0.019* | 1.569 | 1.212 to 3.215 | |
| Warm-up | Yes | Reference group | - | - | - |
| No | 1.159 | 0.011* | 1.406 | 1.092 to 2.919 | |
| Bracing | Yes | Reference group | - | - | - |
| No | 1.450 | 0.006* | 2.163 | 1.219 to 2.979 | |
*Significant at p < 0.05.
Finally, it should be mentioned that to prevent ankle sprains, it is important to employ a multi-disciplinary team approach, involving sports trainers, coaches, physicians, and physical therapists, as well as the players. Raising awareness of the complexity of the situation and improving individual compliance under the supervision of trainers and physical therapists are essential factors. All these factors are important in implementing ankle sprain prevention strategies.
4.1. Limitations
To the best of authors’ knowledge, this is the first study to analyze the prevalence and risk factors of ankle sprain among amateur and professional male soccer players in Tabuk in particular and Saudi Arabia in general. The findings of this study can be expected to contribute to guiding medical and support staff in soccer clubs regarding how to reduce the prevalence of ankle sprain among players. However, this study has some limitations which should be discussed. One limitation is that we did not record the frequency of injury in the dominant side versus the non-dominant side. These recordings could have added important information to the study’s results with respect to the difference in injury occurrence and recurrence between the two sides [53]. Yet, we believe that this limitation does not affect the significance of the major findings of the study about the prevalence and risk factors of an ankle sprain. Another limitation is that the study sample was limited to male soccer players. However, this could have a minimum effect on the generalizability of the results because soccer is uncommonly played among females in Saudi Arabia. Finally, the sample was drawn from a single region in Saudi Arabia, which may also affect the generalizability of the results. However, we believe this study could lead to future studies in other regions of Saudi Arabia.
CONCLUSION
Ankle injuries are the most prevalent among lower limb injuries in Saudi Arabian male soccer players, particularly in the Tabuk region. Previous ankle injuries, lack of stretching, lack of warm-up, and not wearing bracing were the highest risk factors for the occurrence of an ankle sprain. Players had little knowledge of injury prevention and education. Our findings suggest the importance of increasing the awareness of 1) injuries and 2) the proper physical therapy measures. This might assist in reducing the likelihood of recurrence of ankle sprain injuries among male soccer players.
LIST OF ABBREVIATION
| BMI | = Body Mass Index. |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study was approved by the Research Ethics Committee of the University of Tabuk, Tabuk, Saudi Arabia (Approval No. UT-73-21-2018).
HUMAN AND ANIMAL RIGHTS
No animals were used for this study. All research procedures in this study were performed in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national).
CONSENT FOR PUBLICATION
Written informed consent was obtained from each participant.
STANDARD OF REPORTING
Strobe guidelines and methodologirs were followed.
AVAILABILITY OF DATA AND MATERIALS
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
FUNDING
None.
CONFLICT OF INTEREST
The author declares no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
We would like to acknowledge the support of all of the soccer players who participated in the study and the physical therapy students at the University of Tabuk who helped with data collection.
SUPPORTIVE/SUPPLEMENTARY MATERIAL
Self-Structured Questionnaire.

