All published articles of this journal are available on ScienceDirect.

Effects of Traditional Strength Training Versus Jump Training on Muscular Fitness among Physically Inactive and Sedentary Young Adults
Authors Info & Affiliations
Abstract
Background:
The effects of Traditional Resistance Training (TRT) and Plyometric Jump Training (PJT) had never been compared in participants that are both sedentary and physically inactive. Results derived from such research may allow important practical applications.
Objective:
The aim of this study was to compare the effects of 4-weeks of TRT versus PJT programs on the muscular fitness of sedentary and physically inactive participants.
Methods:
Baseline and follow-up tests included the assessment of Squat Jump (SJ), Countermovement Jump (CMJ), elastic index, and maximal strength of the knee extensors (MVS). Males and females (age range, 18-29 years) were randomly assorted into a control group (CG, n=11), TRT (n=8), and PJT groups (n=9). The TRT program emphasized slow-speed movements with free weights. The PJT program emphasized high-speed jump movements without external loads. Both TRT and PJT sessions lasted 30-minutes. Dependent variables were analyzed in separate three (Groups) × two (Time: pre, post) ANOVA, with Bonferroni-adjusted α (p<0.05).
Results:
Main effects of time (all p<0.05) were observed for SJ (ηp2 = 0.51), CMJ (ηp2 = 0.33), and MVS (ηp2 = 0.33). Post-hoc analyses revealed similar significant (all p<0.05) improvements in the TRT and PJT groups for SJ (∆, 95%CL, 9.0-22.5%), CMJ (∆, 95%CL, 11.7-24.4%), and MVS (∆, 95%CL, 5.8-21.3%). No significant changes were observed in the control group. No changes were observed for the elastic index.
Conclusion:
In otherwise healthy participants that are both physically inactive and sedentary, both TRT and PJT protocols are equally effective in improving the muscular fitness.
1. INTRODUCTION
Competent levels of strength and power (muscular fitness) are required to perform a range of movements with precision and confidence in a variety of athletic scenarios [1]. Habitual development of these qualities may improve health and fitness, enhance physical performance, reduce the relative risk of injury, and develop confidence and competence [1]. Moreover, poor muscular fitness is associated with mortality [2], cardiovascular disease [3], among other health markers [4], with recent findings demonstrating an alarming trend towards reduced muscular fitness in young population over the years [5], a reduction that showed accelerated rates in recent decades [6].
Traditional resistance training (TRT) and plyometric jump training (PJT) are effective means of physical conditioning for muscular fitness, promoting improvements in skill-related measures of physical performance, as well as in health (i.e. bone health) and resistance to injury [7, 8]. To implement effective TRT and PJT programs, several key programming characteristics should be considered, such as the overload principle, the volume and intensity of prescribed drills, and the order of within-session drill execution, among others (i.e., training surface [7-9].
However, in addition to TRT and PJT configuration, the characteristics of program participants should also be considered to optimize adaptive responses in strength and power [10]. Although the benefits or TRT on strength and power have long been confirmed in sedentary and physically inactive participants, for both female and male participants [8], a recent scoping review on PJT [11], from 242 reviewed articles, reported that only ~8% were conducted in participants with low physical fitness (e.g., sedentary or physically inactive participants). It may be that due to the acute muscle-damaging effects of PJT, practitioners and researchers are reluctant to implement PJT in participants with low physical fitness levels. However, recent literature has demonstrated its efficacy in different health-related contexts [12] indicating the use of the method in non-athletic populations. Despite this, no study has thus far compared the effectiveness of TRT and PJT on the muscular fitness (i.e., maximal strength and muscle power) responses in participants that are both sedentary and physically inactive. There is evidence linking physical inactivity and sedentary behavior, independently [13], to increased risk of adverse health outcomes, including type two diabetes, cardiovascular disease and all- and specific-cause mortality. Thus, practical and effective training interventions are required in ‘at-risk’ populations.
Although the benefits of TRT for individuals with unhealthy habits (sedentary and physically inactive) have been reported on muscle strength and power [8], the potential benefits of PJT still need to be confirmed in this group of the population. Previous studies argued that when jumping exercises are introduced into the training schedule, an initial strength training base should be introduced first [14], although this contention has been disputed [15]. In fact, the stretch forces that occur during plyometric movements give rise to eccentric muscle actions. The resultant stored elastic energy and activation of the stretch reflex contribute to potentiation of elastic force, with greater neural excitation in subsequent concentric actions, a mechanism termed the stretch-shortening cycle (SSC) [9]. An individual’s ability to leverage this mechanism is an important determinant of optimal muscular performance, influencing abilities in strength [16] and jumping [17]. Moreover, a meta-analysis observed that maximal strength may be increased after PJT, independent of initial strength training base [18]. Therefore, it is assumable that both, TRT and PJT may be capable of inducing improvements in both maximal strength and power in sedentary and physically inactive participants.
Although the implementation of TRT is effective, its practical application is questionable, especially for larger groups which may require the use of extensive equipment and physical space. On the contrary, the effective [7, 9] implementation of PJT programs requires almost no equipment and very little space, and requiring relatively little time to be completed. This is a major determinant of sustained engagement in a physically active lifestyle for college-age participants [19]. Moreover, when TRT and high-speed resistance training (including PJT drills) programs are compared, usually, the latter show a greater adherence rate [20]. Unfortunately, no randomized controlled trial has yet compared the effectiveness of TRT and PJT programs on the muscular fitness (i.e., maximal strength and muscle power) response of participants that are both sedentary and physically inactive. Therefore, the aim of this study was to compare the effects of TRT and PJT programs on the muscular fitness responses in participants that are both sedentary and physically inactive. We hypothesized that, compared to TRT, a PJT program would be equally effective to enhance the muscular fitness (i.e., maximal strength and muscle power) of sedentary and physically inactive male and female participants. Muscle power was considered as a primary outcome, and maximal strength as the secondary outcome.
2. MATERIALS AND METHODS
2.1. Participants
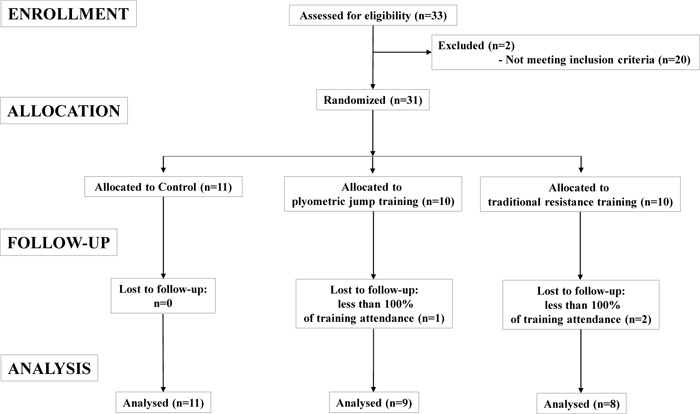
The following eligibility criteria were applied: (i) no musculoskeletal injuries for the last 2 months prior to the start of the study, (ii) no medical problems that could compromise study participation (including cardiovascular disease), (iii) no lower-extremity surgery during the previous 2 years, (iv) being both sedentary and physically inactive [13], thus without systematic PJT or TRT experience during the previous 12 months prior to their recruitment into this study, (v) ability to jump with maximal effort, (vi) body mass index (BMI) <30 kg.m-2. Sedentary behavior was determined according to previous criteria for the population from the country where the study was conducted. Briefly, participants were considered sedentary if they reported ≥8 hours per day spent in sedentary activities (i.e., those requiring <1.5 METSs) [21]. From advertisement in a local university, thirty-three subjects volunteer to participate in the study. From these, two were unable to participate due to a lack of conformity with the eligibility criteria. The remaining thirty-one subjects were randomly assigned to PJT, TRT and control groups. After completion of the intervention, another three subjects (PJT, n=1; RT, n=2) were removed from the study because they did not follow the targeted adherence rate (i.e., had more than three absences from training). Therefore, twenty-eight physically-inactive and sedentary young males and females participated in this study. An active control group and an experimental group that followed standardized nutrition to control for potential effects of changes in physical activity, sedentary behavior and dietary habits were not possible. To rule out these potential sources of bias, we standardized physical activity, sedentary behavior and diet over the course of the study by asking the subjects to maintain their physical activity, sedentary status and diet throughout the intervention.
Participants were randomly allocated into a control group (CG, n=11 [six females]; age, 23.6±2.4 years; BMI, 23.5±3.7 kg.m-2), resistance training group (TRT, n=8 [five females]; age, 22.6±2.9 years; BMI, 22.4±2.2 kg.m-2), and a plyometric training group (PJT, n=9 [five females]; age, 22.2±1.7 years; BMI, 22.8±3.1 kg.m-2). To calculate the sample size, statistical software (GPower; University of Dusseldorf, Dusseldorf, Germany) was used. Given the study design (3 groups, 2 repeated measures), a conservative effect size = 0.4, alpha-error <0.05, nonsphericity correction € = 1, correlation between repeated measures = 0.5, and desired power (1-ß error) = 0.8, the total sample size resulted in 21 participants. Considering a 25% drop out rate, the minimal total sample size was set at 27 participants.
This study was carried out in accordance with the recommendations of the latest Declaration of Helsinki, and was approved by the review board from the *blind for review purposes*. Participants were informed about the experimental procedures and possible harms and benefits before the start of the study. Written informed consent was obtained from all participants before the beginning of the study. A CONSORT diagram of participant’s recruitment, allocation, follow-up and analysis is indicated in Fig.(1).
2.2. Measurements
Stature and body mass were measured using a stadiometer to the nearest 0.1 cm and 0.1 kg, respectively (Adam, model MDW 160M; Adam Equipment Co. Ltd.; Maidstone Road, Kingston, Milton Keynes, MK10 0BD, UK).
Maximal strength of the dominant leg (i.e., determined by asking the participant the preferred leg used to kick a ball) knee extensor muscles was measured using a dynamometer (Art-oficio equipment, model FMON-1, Santiago, Chile) with a precision of 0.25 N. The validity of the equipment and the reliability of the protocol have previously been documented [22]. Briefly, the participant sat upright in a knee-extensor machine, with a 90° knee angle (0° = full knee extension), and was restrained firmly with straps at the chest, waist, and thighs. The ankle pads were placed just above the lateral malleoli. The participant was instructed to maintain the maximal effort for ~3 seconds before relaxing, with 60 seconds of rest between efforts. The largest of the three maximal efforts obtained at each time point was used in subsequent analyses.
The countermovement jump and the squat jump tests were performed according to previous recommendations, using a validated mobile app [23] (app “My Jump 2” for the iPhone 6). Briefly, during the squat jump, participants adopted a flexed knee position (~90°) for 3 seconds, followed by a maximal concentric-dominant effort vertical jump. During the countermovement jump, the participant performed a downward movement with no restriction imposed over the knee angle achieved, followed by a vertical jump. The feet of the participants were focused on using the iPhone 6’s zoom function. All jump values were transformed into Watts according to a previously validated equation [24]. Additionally, as previously described [25], the elastic index, was assessed as a relative value of CMJ over that achieved in the SJ, with the index calculated as: [(countermovement jump × 100)/squat jump]-100.
2.3. Training Protocols
While the participants from the CG continued with their habitual daily activities, both training groups trained on Monday, Wednesday and Friday over 4 weeks. This intervention period is commonly used [9] to induce significant improvements in different types of muscular fitness parameters, including jumping and strength parameters. Each training session lasted ~30 minutes, supervised by one of the lead researchers. Each training session also included a warm-up and cool-down period.
The TRT program was formulated based on previous recommendations [8] and included squat, box step up, front squat, and split squat exercises, all performed with free weights. Considering the difficulty in performing one repetition maximum assessment for all these exercises, a repetition maximum continuum was used for load prescription during TRT. In this sense, a given number of repetitions for a given set and exercise was used, in line with its excepted result in very specific training adaptations (i.e., power; strength), according to its expected relation to given intensities [26]. Participants completed three sets of ten repetitions during the 1st week, four sets of eight repetitions during the 2nd week, three sets of six repetitions during the 3rd week, and four sets of four repetitions during the 4th week. The rigorous technique was maintained during all exercises, under the direct supervision of a strength and conditioning coach. Participants were instructed to use the highest weight possible, whilst also demonstrating sound technique, for the prescribed number of sets of each exercise during each training session. To accomplish the training principle of overload, the resistance was increased (i.e., 1-5%) when the participant was able to lift the prescribed repetitions for the final set of a given exercise. In this way, training to muscle failure rarely occurred, the exception being during the final set in some training sessions. Thus, although baseline one repetition maximum values were neither determined nor adjusted, the progressive overload system used (i.e., repetitions-based intensity) allowed the adjustment of training loads (i.e., weights) proportionally to changes in maximal strength. All repetitions during the TRT program were performed with controlled speed (i.e., ~2-3 seconds for the concentric and eccentric portion of the movements). Participants recovered for 60 seconds between sets and 20 seconds between exercises.
The PJT program is described in Table 1. Plyometric jump training was immediately performed after the warm-up program [27]. The PJT protocol was formulated based on previous research findings and recommendations [9]. The order of execution for the different drills in a given week were randomized for each session [28]. Bilateral, unilateral, non-repetitive, repetitive, horizontal, vertical, lateral, diagonal, involving slow (≥250-ms) and fast (<250-ms) SSC movements were incorporated. For all PJT groups, a strong emphasis was put on sound landing technique and shock absorption, using a medium to hard training surface [29, 30]. The participants in the PJT group were asked to jump at maximal effort (i.e., minimal contact time with the ground, maximal jump distance-height, or a combination of both for maximal reactive strength performance). To ensure that subjects achieved the desired intensity during each jump, a coach-to-subject ratio of 1:1 was used during all training sessions. The coach supervised each jump and was attentive to the intensity and technical skill level of execution. A rest period of ~5 seconds was granted between repetitions, and 120 seconds was given between sets [31]. For the repetitive jumps, no rest between jumps was required. Each PJT session included four to five PJT drills, with two to five sets per drill, and six to twenty repetitions per set. The volume of training was increased progressively [32], from the 1st to the 4th week of training. All PJT sessions lasted 30-minutes, for a total of ~2,211 jumps during the entire program. The PJT sessions were scheduled between 16.00 to 20.00 hrs.
Considering the difficulty in equalizing TRT and PJT programs loads due to their different nature, in the current study, a more practical approach was used, taking into account the sedentary and physically inactive level of the participants, and the lack of time during the day as the major limitation to adopt a more active lifestyle. In this sense, both TRT and PJT groups were equalized for a total time of training (i.e., 30 minutes per session).
| Week | Drill | Sets x repetitions |
| 1 | Side to side ankle hops Standing jump and reach Front cone (~20 cm) hops Squat jump |
2x15 2x15 5x6 3x15 |
| 2 | Side to side ankle hops Standing long jump Lateral jump over barrier (~30 cm) Squat jump |
2x15 5x6 2x12 3x15 |
| 3 | Side to side ankle hops Standing long jump Lateral jump over barrier (~30 cm) Squat jump Single leg bounding |
2x20 4x8 4x15 4x15 4x10 |
| 4 | Lateral cone (~20 cm) hops Diagonal cone (~20 cm) hops Split squat jump Squat jump with 5 kg Tuck jump with knees up |
4x10 3x20 4x10 4x15 4x10 |
| - | Control group (n=11) | RT group (n=8) | PJT group (n=9) | ANOVA outcomes | |||||
| Group F(2, 25), p-value (ηp2) |
Time F(1, 25), p-value (ηp2) |
Group x Time F(2, 25), p-value (ηp2) |
|||||||
| - | Pre | Post | Pre | Post | Pre | Post | |||
| Countermovement jump (W) | 866±326 | 869±179 | 967±328 | 1115±355a | 911±211 | 1076±210b | F=1.2, p=0.3 (0.1) | F=12.1, p<0.05 (0.33) | F=3.2, p=0.05 (0.21) |
| Squat jump (W) | 732±149 | 767±167 | 837±265 | 974±316b | 834±195 | 941±159a | F=1.7, p=0.2 (0.1) | F=26.2, p<0.05 (0.51) | F=2.9, p=0.07 (0.19) |
| Elastic index (%)* | 16.8±28.1 | 13.9±7.6 | 16.5±15.6 | 15.6±12.9 | 9.3±8.8 | 14.0±6.3 | F=0.42, p=0.7 (0.0) | F=0.1, p=0.9 (0.0) | F=0.3, p=0.8, (0.1) |
| Knee extensors strength (N) | 326±68.4 | 367±74.0 | 327±68.1 | 415±85.0a | 335±79.5 | 381±86.0a | F=2.1, p=0.2 (0.1) | F=12.4, p<0.05 (0.33) | F=1.0, p=0.5 (0.1) |
2.4. Statistical Analysis
Data are presented as group mean values ± standard deviations. Normality and homoscedasticity assumptions were checked with the Shapiro-Wilk and Levene’s tests, respectively. For nonparametric outcomes (i.e., CMJ power), data were log-transformed for analysis to reduce bias arising from non-uniformity error and were back-transformed for presentation purposes. Analyses of variance (ANOVA) were used to detect between-group differences in all variables at baseline and follow-up. Measures of dependent variables were analyzed in separate three (groups) × two (time: pre, post) ANOVA with repeated measures on time. Post-hoc tests with Bonferroni-adjusted α were conducted to identify comparisons that were statistically significant. Effect sizes were determined by calculating partial eta-squared derived from ANOVA analysis. Statistical analyses were carried out using STATISTICA statistical package (Version 8.0; StatSoft, Inc, Tulsa, United States). Significance was set at an alpha level of p<0.05. To assess reliability, thresholds of ≥0.80 for the intra-class correlation coefficient were set.
3. RESULTS
All participants received treatment as allocated. No test or training-related injuries occurred over the course of the study (assessed by self-report in a session-by-season manner). All groups reported no changes in their daily habits during the 4 weeks of the intervention, as compared to their habits prior to recruitment.
No significant between-group baseline differences were observed for any fitness or descriptive measurements. The main effects of group, time, and group × time interactions are displayed in Table 2.
Significant main effects of time were observed for countermovement jump, squat jump, and maximal strength (all p<0.05; d=0.33-0.51) (Table 2). No significant group × time interaction effects were observed for countermovement jump (p=0.05; d=0.21), squat jump (p=0.07; d=0.19), and knee extensors maximal isometric strength (p=0.5; d=0.1) (Table 2).
Post-hoc analyses revealed significant improvements in the TRT group for countermovement jump (p=0.014, ∆15.3%, 95% CL 4.0-28.7%), squat jump (p=0.0064, ∆16.3%, 95% CL 3.1-31.2%), and knee extensors maximal isometric strength (p=0.035, ∆11.5%, 95% CL -3.0-27.9%). Similarly, post-hoc analyses revealed significant improvements in the PJT group for countermovement jump (p=0.0045, ∆18.2%, 95% CL 11.6-27.5%), squat jump (p=0.038, ∆12.8%, 95% CL 6.9- 22.0%), and knee extensors maximal isometric strength (p=0.019, ∆13.6%, 95% CL 4.9-24.1%). No significant changes were observed for the CG in countermovement jump, squat jump, or knee extensors maximal isometric strength (p>0.05). The improvements for the countermovement jump, squat jump, and knee extensors maximal isometric strength were no significant difference between the traditional resistance training group and the plyometric training group. No group, time or time x group interactions were observed for the elastic index.
4. DISCUSSION
The aim of this study was to compare the effects of TRT and PJT programs on the muscular fitness responses in participants that are both sedentary and physically inactive. According to our hypothesis, compared to TRT, a PJT program was equally effective to enhance maximal strength and muscle power of sedentary and physically inactive male and female participants. Specifically, the main effects of time were observed for countermovement jump, squat jump and maximal voluntary strength. Post-hoc analyses revealed similar significant improvements in the TRT and PJT groups for CMJ, SJ, and MVS, while no significant changes were observed for the CG. No group, time or group×time interactions were observed for the elastic index. Therefore, both TRT and PJT are equally effective in improving the muscular fitness (i.e., maximal strength and muscle power) in participants that are both sedentary and physically inactive.
The improvements in CMJ in sedentary and physically inactive participants in this study after TRT or PJT, are similar in magnitude when compared to previous studies conducted in other populations of either physical inactive or sedentary participants. In a study conducted in sedentary, males (aged ~21 years) saw an improvement in the vertical jump (d=0.63-0.85) after twelve training sessions in a 6 week period, totaling 1,200 jumps over the course of the intervention [33]. Additionally, a study conducted in sedentary males and females (aged ~19 years) found an improvement in the vertical jump of ~22% after sixteen training sessions over 8 weeks of training using a combined TRT and PJT program [34]. Increases in jumping ability are likely related to enhanced neural drive, improvements in the stretch reflex, increased re-utilization of stored elastic energy, improved muscle activation strategies with greater motor-unit recruitment, and better inter- and intra-muscular coordination, as well as possible improvements in muscle size and/or architecture, and single-fiber mechanics [7, 35]. Such adaptations in physically inactive and sedentary participants may aid in their ability to perform a range of movements with precision and confidence in a variety of scenarios [1]. This can facilitate the improvement of health and fitness, enhance physical performance, reduce the relative risk of injury, and develop confidence and competence [1] in trainees, potentially leading toward reduced mortality [2], cardiovascular disease [3], among other health-markers improvements [4].
Likewise, the improvement in SJ after a PJT might be expected since some previous studies have reported positive results in this test among adults [36]. Although it is tempting to postulate that the untrained nature of the participants in the current study may be accounted for the observed results, several reviews and meta-analyses have failed to prove a moderating effect of participants’ initial fitness level on vertical jump improvements after a PJT intervention [10, 36]. On this basis, the merit of the current training approaches in the population in question should not be underestimated. Further to this, although the initial fitness level of the participants must be considered for adequate training prescription and progression to be applied [8], current findings demonstrate that, as with TRT programs, PJT may be implemented effectively for sedentary and physically inactive adults who are unaccustomed to this type of exercise. Practitioners should, nonetheless, adopt a cautious approach to training prescription but can progress both volume and intensity as the trainee attains proficiency [12]. Of note, as in the current investigation, the use of 4 weeks of training to induce improvements in jumping ability seems common [9]. Such rapid increases in functional power may be relevant to motivate sedentary and physically inactive participants from an early stage of training when a lack of progress could be relatively more detrimental to the continued uptake of physical activity. Such rapid muscle power improvements may facilitate an early increase in spontaneous physically activity or reduced sedentary behavior, potentially favoring key metabolic and cardiovascular risk markers. While more long term evidence is needed to substantiate this point, PJT seems to be a viable training option at the beginning of a program in sedentary and physically inactive people.
To monitor muscular fitness, the CMJ and the SJ are commonly used, with jump performance usually greater in the former compared to the latter type of jump movement. Such phenomena were reported as early as in the year 1895 [37], and possibly reflect the complex neuromechanical mechanisms involved in the SSC [35]. Additionally, the relative difference between the CMJ and the SJ is commonly named elastic index, a potential indirect indicator of the elastic phenomena involved in the SSC [25]. Although the description of the elastic index is relatively common and data from the nineteenth century, no study has compared, until now, the effects of TRT and PJT on this index in physically inactive and sedentary participants. Current findings suggest that neither training method had a significant effect on the elastic index. In other words, although muscular fitness (maximal strength and power) can be improved with TRT and PJT, the elastic index is not significantly changed, probably due to the similar relative increase in CMJ and SJ performance. In this sense, a larger difference between the jumps (i.e., greater elastic index) is not necessarily a better indicator of muscular fitness (high-intensity sports performance) [38].
Regarding MVS, the TRT and the PJT groups improved their voluntary isometric maximal knee extensor strength after 4 weeks of training. This finding is similar to that previously reported for a group of young (~25 years) untrained healthy males [39]. In the aforementioned study both TRT (~29%) and PJT (~22%) groups achieved similar gains in maximal strength with the authors reporting increases in maximal leg press strength. Notably, muscle hypertrophy (~7%; hamstring, quadriceps and adductors cross-sectional area) was induced by PJT, with similar increases for the TRT group [39]. However, the aforementioned study lasted 12 weeks and whether or not similarly large increases in hypertrophy can be induced in as little as 4 weeks, is yet to be proven. Nevertheless, it is possible that rapid (< 4 weeks) adaptations occurred after the current PJT (and TRT) interventions, as PJT seems to be an effective strategy to improve maximal strength in relatively short periods of time [16], probably due to neuro-musculoskeletal adaptations [7]. However, it must be noticed that the aforementioned study of Vissing et al. [39] did not incorporate a control group and was conducted only in male participants. Furthermore, it was not clear if the participants were sedentary, physically inactive or a combination of both. Therefore, the current findings offer novel insights and expand the limited knowledge available with regard to the effects of PJT on muscle performance of sedentary and physically inactive participants, after a 4 week intervention.
The lack of adverse responses to PJT among (healthy) participants that are both sedentary and physically inactive, is encouraging. Although current evidence points toward the safety of PJT exercise in this population, practitioners should take a cautious approach to programming. In addition, the reader must consider the lack of uniformity in how training programmes are prescribed in the literature. Practitioners are advised to take general guidelines to formulate PJT programmes according to the current scientific evidence and make them appropriate to the individual(s) with whom they are working [40-43]. In future studies, researchers are encouraged to describe how data related to injury, pain or any other potential adverse effect was collected, clarifying the procedures, definitions, diagnosis by a qualified medical practitioner, among other key aspects.
In the current study, a high-quality (e.g., randomized-controlled) research protocol was used, allowing novel findings, related to the similar improvement of muscle power and strength in young males and females after TRT or PJT. Such findings may have important applications in clinical and sport-related settings. However, the short-term nature (4 weeks) of the intervention limits the possibility of establishing if the temporal pattern of improvements would continue or vary in an interconnected fashion. In addition, the age (18-29 years) and relatively small sample size (n=28) may limit the generalizability of current findings. Moreover, future studies may incorporate mechanistic insights into the potential physiological, anatomical, biomechanical factors related to the observed improvements.
CONCLUSION
Both TRT and PJT are equally effective in improving the muscular fitness (i.e., maximal strength and muscle power) in otherwise healthy participants that are both sedentary and physically inactive. Considering the relatively low cost, easiness of implementation, and effectiveness of PJT, it may offer an alternative to TRT programs for sedentary and physically inactive participants.
LIST OF ABBREVIATIONS
| ANOVA | = Analysis of Variance |
| BMI | = Body Mass Index |
| CG | = Control Group |
| CMJ | = Countermovement Jump |
| MVS | = Maximal Voluntary Strength |
| PJT | = Plyometric Jump Training |
| RT | = Resistance Training |
| SJ | = Squat Jump |
| SSC | = Stretch-Shortening Cycle |
| TRT | = Resistance Training Group |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The approval of the ethical committee with a reference number of approval 004-2019 provided by the Ethical Committee of the Department of Physical Activity Sciences, University of Los Lagos.
HUMAN AND ANIMAL RIGHTS
All research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the latest version of the Helsinki Declaration.
CONSENT FOR PUBLICATION
Not applicable.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article is available upon request to the corresponding author (Rodrigo Ramirez-Campillo).
FUNDING
None.
CONFLICT OF INTERESTS
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
We are gratefully with all the participants that volunteered in this study.

