All published articles of this journal are available on ScienceDirect.

A Comparison of Injuries in Different Non-Professional Soccer Settings: Incidence Rates, Causes and Characteristics
Authors Info & Affiliations
Abstract
Background:
There is a lack of data regarding the epidemiology of soccer injuries and the particular accidents in specific non-professional soccer populations. The aim of this study was to analyse incidence, causes and characteristics of soccer injuries, taking into account different settings of organised (amateur) and non-organised soccer.
Methods:
A random sample of persons who had sustained an injury while playing soccer and reported this injury to the Swiss National Accident Insurance Fund (Suva) was retrospectively consulted. 705 injuries were analysed involving three main settings (soccer games, soccer training, non-organised soccer) and different amateur soccer leagues.
Results:
Knee injuries (p=0.01) and head injuries (p=0.005) were observed more frequently in games than in non-organised soccer. Injuries caused by contact with an opponent and foul play occurred more frequently in games than in training (p<0.001) or non-organised soccer (p≤0.001). Injury incidence was substantially higher for players of 30+/40+ leagues (18.7 injuries per 1000 hours) than for players of other leagues (1st-3rd amateur leagues: 8.5, p=0.002; 4th-5th amateur leagues: 9.4, p=0.007; female leagues: 8.2, p=0.006; junior leagues: 6.7, p<0.001).
Conclusion:
With respect to injury characteristics, causes and injury incidence, essential differences between various non-professional soccer settings exist suggesting that a more specific approach in injury prevention may generate positive effects.
1. INTRODUCTION
Soccer is the most popular team sport in Switzerland [1]. Amongst the 15- to 74-year-old population, about 480,000 persons play soccer, which corresponds to a percentage of 7.8% of this population [2]. Of these, 190,000 individuals participate in official championships. According to international studies, the overall injury incidence for competitive amateur soccer players ranges from 5.2 to 9.6 per 1000 hours of play [3-5]. Prior research has compared incidence rates in amateur and professional soccer, yielding inconsistent findings. While van Beijsterveldt et al. [6] compared an amateur cohort to a professional one and found a higher injury incidence in amateur soccer players including an increased risk for moderate and severe injuries, other studies reported a lower [7] or comparable [8] injury risk for specific amateur soccer populations compared with professional players. Given the high number of players involved in amateur soccer and the high injury risk, it is perhaps surprising that only a few investigations have provided information about the circumstances leading to injuries in this setting. For instance, previous studies have shown that - as in professional soccer - player to player contact is a frequent injury mechanism in amateur soccer games, causing more than half of all injuries [4, 9]. In training however, non-contact injuries seem to be more common than injuries due to player contact. Interestingly, the frequency of contact injuries does not vary between high- and low-level players when only severe injuries are considered [10].
With regard to the contributing factors which lead to injuries in amateur soccer, contact with another player is the most frequent injury mechanism followed by distortion and turning/twisting [5]. Moreover, in their review on incidence and prevention of soccer injuries Junge and Dvorak [11] found that 12% to 28% of all injuries were caused by foul play. However, this review was not exclusively focussed on amateur soccer. These data accord well with another investigation with players of different skill levels, in which almost 30% of traumatic injuries were associated with foul play [12].
Despite these findings, it should be noted that amateur soccer is not a homogenous setting. Only a few studies have factored in various levels of amateur soccer, and these have found contradicting results. Peterson et al. [12] compared players from all levels (including top level) and concluded that while low-level players had lower exposure to soccer, they were more likely to get injured. In contrast, Schmikli et al. [13] identified more skilled adult amateur players as a target group for prevention, because they had an increased injury risk. Hammes et al. [8] exclusively focussed on veterans (aged 32 or older) who played competitively in a separate league. They found an injury incidence that was comparable to other male soccer levels, but injury characteristics were different. In summary, these finding clearly underline the importance of research within different amateur soccer populations.
Finally, besides competitive amateur soccer, a high number of people play soccer non-organised. Of the 15- to 74-year-old Swiss population, 290,000 persons practice soccer outside of clubs and official championships [2]. To the best of our knowledge, no studies exist so far with regard to the epidemiology of soccer injuries in non-organised settings. Taken together, we suggest that there is a lack of data regarding soccer accidents in specific non-professional soccer populations. Therefore, the aim of the present study was to analyse and compare incidence, causes and characteristics of injuries in different settings of organised and non-organised non-professional soccer.
2. MATERIALS AND METHODS
2.1. Procedure
A retrospective telephone survey of people who were injured while playing soccer was carried out in 2014. Annually, 45,000 soccer accidents affecting working people are counted in Switzerland of which 30,000 are recorded by the Swiss National Accident Insurance Fund (Suva) [14]. Of these, a random sample of 2835 persons was drawn with the aim of interviewing approximately 800 persons.
The selected persons were initially contacted by an information letter including an informed consent form. For those who did not respond, a second attempt was made by phone. This process was stopped when a total of 1055 (37.2%) persons had given their written or oral consent what allowed to conduct 822 interviews (participation rate: 77.9%). An interview took 16 minutes on average. All participants had sustained a soccer injury between July 2013 and June 2014. To reduce the interval between the accident and the interview, the survey was conducted in two phases. On average, 6 months had passed between the accident and the interview.
2.2. Data Screening and Final Sample
For not reporting a soccer injury three persons were directly excluded. Comparing the respondents with the rest of the random sample, a small selection bias was identified with respect to gender (p<0.001) and nationality (p=0.002), with the participation rate being higher among women (5.8% vs. 3.0%) and Swiss citizens (78.6% vs. 73.0%). No differences were found with regard to age (p>0.05). In several cases, the type of injury described did not correspond with the information provided by the Suva data pool. Thus, 69 participants referred to another registered soccer accident and 42 to an unregistered injury. Moreover, three participants did not provide details on the injury setting. All these participants were excluded from all further analyses, resulting in a final sample of 705 participants.
2.3. Definitions and Questionnaire
Only injuries which required medical attention were considered. The classification of injury severity was based on the number of days until the player could practice sports as he did before the injury. The participants were asked whether their injury was caused by contact and by foul play, and they had to specify the referee’s decision. Additionally, the participants were asked to describe the injury situation more precisely, which allowed distinguishing 19 different injury categories based on the work of Hawkins et al. [15] Injury incidence was defined as the number of injuries per 1000 playing hours. Therefore, all participants were asked about the number of injuries they had suffered during the past year. Furthermore, participants playing in a soccer club were asked how many hours per week they had played soccer. To obtain an estimate of the exposure time throughout a year, the weekly playing hours were multiplied by 40 weeks. Finally, the respondents had to answer questions about their preventive behaviour prior to the injury.
2.4. Statistical Analysis
All analyses were performed using SPSS Statistics software (version 22.0). Three main soccer settings were compared: games (i.e. persons who were injured during games with their soccer club team), training (i.e. persons who were injured during practice with their soccer club team), non-organised (i.e. persons who were injured while playing recreational soccer with family and friends or a fun tournament). To examine differences between these three settings, χ2 statistics were applied for nominal variables, and t-tests for continuous variables, whereby the significance level was set at p<0.017 due to Bonferroni correction. For categorical variables, the Kruskal-Wallis test was used (using pairwise comparison function). The χ2 statistics were also used to identify general differences between leagues and non-organised settings (significance level at p≤0.05) and to compare groups of leagues pairwise (significance level at p≤0.003 due to Bonferroni correction). With respect to injury incidence, a one-way ANOVA including a Games Howell post-hoc test was conducted (because the homogeneity of variances assumption was not met) to examine differences between groups of leagues. In tables and figures, 95% confidence intervals (95%-CI) are provided.
3. RESULTS
Of the 705 reported injuries, 48.9% (n=345) happened during organised soccer games, 21.0% (n=148) during organised soccer training, and 30.1% (n=212) during non-organised soccer play. Out of the injuries which occurred during non-organised soccer, 61.3% (n=130) occurred while playing with family or friends, 19.3% (n=41) during fun tournaments, 7.5% (n=16) in other sport clubs, 4.2% (n=9) at school, 3.3% (n=7) in alternative leagues, and 4.2% (n=9) in other settings. Whether or not a soccer accident happened in an organised or non-organised context was not associated with the severity of the injury (p>0.05). The distribution of injury setting by gender and age is shown in Table 1. Participants who were injured during a game were on average 26.3 (SD=9.2) years old and somewhat younger than participants who were injured during training (M=29.0, SD=10.9, p=0.008) or during non-organised soccer (M=30.5, SD=11.7, p<0.001). 6.1% (n=43) of the injuries affected a female player. No significant gender differences were found with respect to the three main injury settings (p>0.05). Unlike injury type (p>0.05), injury location was influenced by the setting (p=0.007). In particular, differences were identified concerning knee injuries (p=0.032), head injuries (p=0.010), and thigh and upper leg injuries (p=0.019). While a higher percentage of knee injuries was identified during games (28.1%) compared to non-organised soccer play (18.4%, p=0.010), the number of knee injuries in training (26.4%) did not significantly differ from the other settings (p>0.05). Additionally, there was a higher percentage of head injuries in games (9.0%) than in non-organised soccer (2.8%, p=0.005), but again no difference was found with respect to training (4.7%, p>0.05). Injuries to the thigh and upper leg occurred more frequently in non-organised soccer (7.1%) than in games (2.3%, p=0.006).
As shown in Table 2, a significantly higher proportion of contact injuries and foul play injuries (subjective appraisal) were identified in games compared to training (p<0.001) or non-organised soccer (p<0.001). Additionally, in games, every fourth injury (27.4%) was caused by a foul play penalised by the referee. When considering game injuries only, there were no significant differences in the proportion of contact injuries between different amateur soccer leagues (p>0.05). However, the number of foul play injuries differed significantly between leagues (subjective appraisal: p=0.031, penalised by the referee: p=0.033). A particularly high foul play rate was found in the 30+ leagues. Focussing on non-organised soccer settings only (playing with family or friends, fun tournaments), no significant difference with respect to contact and foul play injuries was identified (p>0.05).
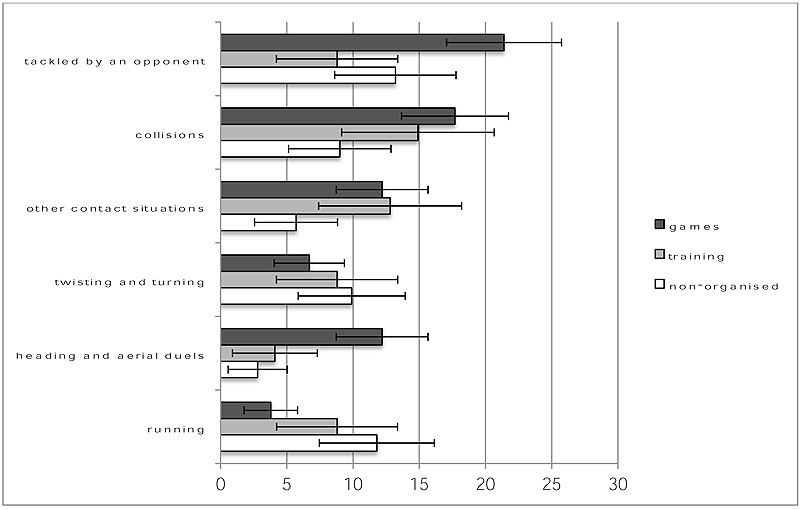
With regard to injury situations, being tackled by an opponent (16.3%, n=115), collisions (14.5%, n=102), other contact situations (10.4%, n=73), twisting and turning (8.1%, n=57), heading and aerial duels (7.7%, n=54), and running (7.2%, n=51) were the most frequently reported situations leading to an injury. As presented in Fig. (1), the most obvious difference with respect to the injury situation appears between games and non-organised soccer. Compared to training and non-organised soccer, in games, more injuries were caused by tacklings by an opponent (training: p=0.001; non-organised soccer: p=0.015) and heading or aerial duels (training: p=0.005; non-organised soccer: p<0.001). While collisions (p=0.004) and other contact injuries (p=0.012) happened more frequently in games than in non-organised soccer, running was a more frequent cause of injury during non-organised soccer play (p<0.001).
The comparison of different groups of amateur leagues yielded significant differences regarding preventive behaviour (Table 3). Players of the 1st-3rd amateur leagues attached more importance to core strength training than players of any other level (p≤0.001), except for women’s leagues (p=0.017). Additionally, players of 30+/40+ leagues stated less frequently that they had performed a core strength training prior to the injury compared to 4th-5th amateur league players (p=0.001). Less than half of all 30+/40+ leagues players had performed a general strength training.
| All Settings | Game | Training | Non-organised | |||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | |
| Gender | ||||||||
| Female | 43 | 100.0 | 27 | 62.8 | 4 | 9.3 | 12 | 27.9 |
| Male | 662 | 100.0 | 345 | 48.9 | 148 | 21.0 | 212 | 30.1 |
| Age | ||||||||
| 15-24 years | 332 | 100.0 | 176 | 53.0 | 79 | 21.1 | 86 | 25.9 |
| 25-34 years | 201 | 100.0 | 116 | 57.7 | 36 | 17.9 | 49 | 24.4 |
| 35-44 years | 97 | 100.0 | 31 | 32.0 | 22 | 22.7 | 44 | 45.4 |
| 45-64 years | 75 | 100.0 | 22 | 29.3 | 20 | 26.7 | 33 | 44.0 |
| Contact injuriesa | Injuries due to foul play (subjective appraisal)b | Injuries due to foul play (penalised by referee)c | |||||
|---|---|---|---|---|---|---|---|
| N | % | 95%-CI | % | 95%-CI | % | 95%-CI | |
| Total | 701 | 52.5 | 49.8-57.2 | 29.4 | 26.0-32.8 | 17.1 | 14.2-20.0 |
| Non-organised | 211 | 37.4 | 30.9-43.9 | 21.0 | 15.5-21.5 | - | - |
| Training | 147 | 36.7 | 28.9-44.5 | 13.8 | 8.2-19.4 | - | - |
| Games | 343 | 69.1 | 64.2-74.0 | 41.2 | 36.0-46.4 | 27.4 | 22.6-32.2 |
| Leagues (only games) d | |||||||
| 2nd amateur leagues | 31 | 64.5 | 47.7-81.3 | 48.4 | 30.8-66.0 | 32.3 | 15.8-48.8 |
| 3rd amateur leagues | 46 | 71.7 | 58.7-84.7 | 42.2 | 27.8-56.6 | 28.9 | 15.7-42.1 |
| 4th amateur leagues | 67 | 70.1 | 59.1-81.1 | 37.9 | 26.2-49.6 | 30.3 | 19.2-41.4 |
| 5th amateur leagues | 44 | 68.2 | 54.4-82.0 | 37.2 | 22.8-51.6 | 19.0 | 7.1-30.9 |
| 30+ leagues | 21 | 81.0 | 64.2-97.8 | 76.2 | 58.0-94.4 | 55.0 | 33.2-76.8 |
| 40+ leagues | 28 | 60.7 | 42.6-78.8 | 35.7 | 18.0-53.4 | 17.9 | 3.7-32.1 |
| Juniors | 49 | 75.5 | 63.5-87.5 | 44.9 | 31.0-58.8 | 34.0 | 20.5-47.5 |
| Women’s leagues | 27 | 81.5 | 66.9-96.1 | 40.7 | 22.2-59.2 | 26.9 | 9.9-43.9 |
| Other | 22 | 45.5 | 24.7-66.3 | 22.7 | 5.2-40.2 | 5.3 | 0.0-15.4 |
| Non-organised settings | |||||||
| Family and friends | 130 | 33.8 | 25.7-41.9 | 18.6 | 11.9-25.3 | - | - |
| Fun turnaments | 41 | 48.8 | 33.5-64.1 | 29.3 | 15.4-43.2 | 20.5 | 5.8-35.2 |
| Others | 40 | 37.5 | 22.5-52.5 | 20.0 | 7.6-32.4 | - | - |
| Core strength training | General strength training | exposure time | Injury incidence per 1000 hours | ||||
|---|---|---|---|---|---|---|---|
| % | 95%-CI | % | 95%-CI | hours/week | inc. | 95%-CI | |
| 1st-3rd amateur leagues (n=127) | 85.9 | 79.8-92.0 | 82.7 | 76.1-89.3 | 6.3 | 8.5 | 7.5-9.6 |
| 4th-5th amateur leagues (n=167) | 68.9 | 61.9-75.9 | 63.5 | 56.2-70.8 | 5.0 | 9.4 | 8.1-11.1 |
| 30+/40+ leagues (n=81) | 46.9 | 36.0-57.8 | 44.4 | 33.6-55.2 | 2.8 | 18.7 | 14.4-23.9 |
| Junior leagues (n=66) | 56.1 | 44.1-68.1 | 71.2 | 60.3-82.1 | 6.3 | 6.7 | 6.0-7.4 |
| Women’s leagues (n=35) | 68.6 | 53.2-84.0 | 74.3 | 59.8-88.8 | 5.4 | 8.2 | 6.0-11.3 |
| Other (n=42) | 55.6 | 41.1-70.1 | 37.8 | 23.6-52.0 | 2.9 | 15.6 | 12.6-18.9 |
In soccer club members, the estimated injury incidence was 10.7 (95%-CI 9.7-11.9) per 1000 hours of soccer play. The injury incidence was highest for 30+/40+ league players with 18.7 injuries per 1000 hours exposure and differed significantly from other males (1st-3rd amateur leagues: p=0.002, 4th-5th amateur leagues: p=0.007), female (p=0.006) and junior (p<0.001) leagues, except for other leagues (p>0.05).
4. DISCUSSION
The major outcome of this study is that substantial differences exist between various non-professional soccer settings with respect to injury characteristics, causes and incidence. A particularly high incidence rate was found among 30+/40+ league players.
For organised soccer players, an incidence rate of 10.7 injuries per 1000 hours of soccer participation was calculated. Even though other studies in amateur [4, 6] and professional [16, 17] soccer found similar or somewhat lower injury rates, a direct comparison of the results is difficult as the present study only included participants who had sustained at least one injury. This may have led to an above average proportion of injury-prone persons and thus an increased injury incidence.
Nevertheless, the presented comparisons between the injury incidences of different amateur soccer leagues should be reliable. Players of 30+/40+ leagues were identified as high-risk group having an increased injury incidence of 18.7 injuries per 1000 hours of play. Based on the fact that players of 30+/40+ leagues had a relatively low exposure time of 2.8 hours per week, it can be assumed that they mainly play in a competitive setting and practice soccer up to once per week. Generally, an increased injury risk in games of veteran soccer players has been reported previously [7], which together with the low training to game ratio leads to an increased overall injury incidence [8]. Hammes et al. [8] calculated a somewhat lower injury incidence of 12.4 injuries per 1000 hours of soccer, because they only included veteran teams (players aged 32 years and older) that performed weekly training sessions, which led to a higher training to game ratio of 2:1. Of particular interest in this context is that players of 30+/40+ leagues reported less frequently that they participated in injury prevention measures compared to players of other leagues. Compared with other levels, physical conditioning is less frequently part of the training sessions in veteran soccer [18]. Thus, adjusted prevention strategies for 30+/40+ league players seem warranted to reduce the high injury risk in this particular group [19].
While injury severity and injury type did not differ between settings (games, training, non-organised soccer), a higher percentage of knee injuries was identified in games compared to non-organised soccer. Considering the fact that knee injuries are predominantly caused without contact12, this difference could be explained by the less competitive character of the game in non-organised soccer which leads to a lower speed and slower changes of direction. Focussing on medical attention injuries in organised amateur soccer, Herrero et al. [7] reported a percentage of knee injuries (29.9%) comparable to our study, whereas Schmikli et al. [13] registered a lower percentage (19.3%), most likely because less severe injuries were also included in their study. Other investigations yielded comparable percentages of knee injuries in amateur soccer (between 15.1% and 24.3%) [6, 9, 20].
Injuries that resulted from contact with an opponent occurred more frequently during games than during training [20] or non-organised playing, which corroborates a higher level of physical play in games of amateur soccer [21]. This leads to a high proportion (41.2%) of injuries caused by foul play in this setting. In our study, more than one quarter of injuries during amateur soccer games happened due to foul play, if the referee’s decision was taken into account. This result is in line with other studies carried out in amateur soccer20 and different levels of professional soccer [11].
Moreover, little is known so far about injury situations in amateur soccer. The present study points out that injuries caused by tackling of an opponent happen more than twice as frequently during games as during training [15], while injuries caused by collisions and other contact situations (pushing, duel without clear ball possession, etc.) occur with a comparable frequency. Injuries caused by heading and aerial duels represent an explicit problem of competitive amateur soccer. Injury situations involving contact with an opponent were significantly less frequent in non-organised soccer. By contrast, a higher amount of injuries were self-inflicted, for example, while running. In summary, although the present study provides preliminary insights regarding the underlying injury mechanisms, more research is needed to gain a more complete understanding of the most relevant factors leading to injuries in different soccer settings and across amateur soccer levels.
4.1. Limitations
A major strength of the present study was that the design allowed a distinction between injuries of players involved in different settings. Despite this strength, several limitations preclude a broad generalisation of the findings. Firstly, the present study exclusively included medical attention injuries, and it was assumed that the respondents correctly reported the diagnosis of their physician. This procedure led to a high number of severe injuries in the present data set. Additionally, it is likely that persons who sustained severe injury were more willing to participate in the present study. Secondly, it is possible that the time period between injury and interview may have caused recall bias. While we acknowledge that injury incidence could thus be underestimated in the present study, retrospective data collection seems to be a suitable method to obtain relevant information about the context and characteristics of an injury [22]. Thirdly, the exposure time was extrapolated based on participants’ statements about the duration of their weekly soccer playing at the time of the injury, which may have led to calculations of injury incidences which are not completely accurate.
CONCLUSION
This study clearly highlights the need for attractive and specific prevention programs addressing players of 30+ and 40+ amateur soccer leagues. Generally, differences in injury causes and characteristics by setting indicate that a more targeted approach of injury prevention is needed. Furthermore, playing competitive amateur soccer involves a higher risk of contact and foul play injuries compared to amateur soccer training or non-organised soccer. Therefore, players, coaches, referees and club officials in amateur soccer need to be more involved in fair play measures to promote a cooperative play.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
No animals/humans were used for studies that are the basis of this research.
CONSENT FOR PUBLICATION
Written informed consent were obtained from all participant.
AVAILABILITY OF DATA AND MATERIALS
Not applicable.
FUNDING
The study was funded and supported by the Swiss National Accident Insurance Fund (Suva).
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declare none.

