All published articles of this journal are available on ScienceDirect.

Shoulder Muscle Activity in Sport Climbing in Naturally Chosen and Corrected Shoulder Positions
Authors Info & Affiliations
Abstract
Objective:
The aim of the study was to determine electromyographic activity of the scapula stabilizing muscles in naturally chosen and corrected shoulder positions in typical static climbing postures.
Methods:
Six male participants undertook surface electromyography measurement in four climbing postures for two different shoulder positions. The activity of the lower, middle and upper trapezius, serratus anterior, pectoralis major, and sternocleidomastoid was recorded. Electromyographic activity was expressed as the percentage of maximal voluntary contraction (MVC) for each muscle.
Results:
Climbing postures induced higher activation of middle and lower trapezius in corrected shoulder positions (35.3 ± 11.8 and 61.7 ± 15.4% MVC respectively) than in naturally chosen shoulder positions (18.4 ± 8.9 and 30.1 ± 13.8% MVC respectively). The highest activity of the middle and lower trapezius was found in postures with the arm in external rotation and 90° abduction and in an overhanging posture. Low activation was stated for the other muscles in both shoulder conditions.
Conclusion:
Results showed that climbers naturally elevate the shoulder during typical static postures. Corrected shoulder positions induce higher activation of the scapula stabilizing muscles than naturally chosen shoulder positions.
INTRODUCTION
Sport climbing is an increasingly popular recreational and competitive activity. The sport is, in contrast to general opinion, relatively safe with an incidence rate of approximately 0.027-4.2 injuries per 1000 hours of climbing [1]. Primarily injuries occur because of chronic overloading, which represent up to 93% of all injuries [2]. Chronic overuse injuries occur due to repetitive stress without adequate rest and are often associated, among other factors, with wrongly performed movement kinematics or, in sport terminology, incorrect technique [3].
Climbers adopt static postures while climbing for route reading, recovery, and to dry the hands with chalk. On steep overhanging walls climbers aim to recover on larger holds, with their arms fully extended at the elbow and with a relaxed shoulder. However, relaxation of the shoulder while hanging is not recommended by clinicians due to the potential for shoulder injury [1]. Common shoulder injuries include superior labral, from anterior to posterior (SLAP), tears and impingements [4]. These two injuries are connected with dysfunctional glenohumeral and scapulothoracic kinematics and weak, or insufficient, stabilising musculature [5]. The main stabilising muscles for the shoulder are the lower and middle trapezius and serratus anterior [6, 7]. Dysfunctional kinematics of the shoulder stabilising muscles while climbing may be associated with changed timing properties of the aforementioned muscles and predominant activation of the upper trapezius. Considering the high incidence of shoulder injuries reported by climbers it would appear that involvement in the sport increases the risk of shoulder injuries, as is the case in many overhead sports [8]. Moreover, large muscle groups such as the pectoralis major and latissimus dorsi are often targeted in climbing training, with the objective of producing gains in strength, subsequently neglecting the stabilising muscles such as the middle and lower trapezius and serratus anterior [9]. It appears that climbers tend naturally to relax their shoulder during static climbing postures, despite active centring of the glenohumeral joint being recommended to prevent muscular imbalance and overuse syndromes [1].
We hypothesised that naturally chosen shoulder positions would induce different activations of the scapula stabilising muscles, in comparison to corrected shoulder positions. The aim of the study was to determine differences in EMG activity for the scapula stabilising muscles in four typical static climbing postures with naturally chosen and corrected shoulder positions.
METHODS
Experimental Approach to the Problem
A two-factor 4 x 2 experimental design with two within-subject factors (static climbing posture x shoulder position) was used to assess the effect of climbing posture and shoulder correction on scapula stabilizing muscles. The dependent variable was the normalized EMG amplitude of m. trapezius (inferior, middle and superior part), m. serratus anterior, m. pectoralis major, and m. sternocleidomastoideus.
Participants
In total, six male participants, right handed, aged between 19 – 36 years volunteered to take part in the study. Three participants (mean age 25.2 yrs, s = 5.3; height 177 cm; s = 1) climbed regularly, at least twice a week. Climbers indicated having completed at least five years of regular specific training and reported red-point climbing abilities from 7b+ to 7c on the Sport grade scale (5.12c – 5.12d Yosemite decimal scale). The climbers took part in the sport 2-3 times per week and completed non-specific climbing exercises such as resistance and/or aerobic training 2-3 times per week. All three climbers practised the sport both outdoors and indoors. The other three participants were recruited from a generally physically active population of non-climbers (mean age 24.2 yrs, s = 1.3; height 189 cm; s = 3). Non-climbing participants reported regular aerobic or resistance exercise 1-2 times per week at a recreational level, and had no experience with either indoor or outdoor climbing.
EMG Measurement
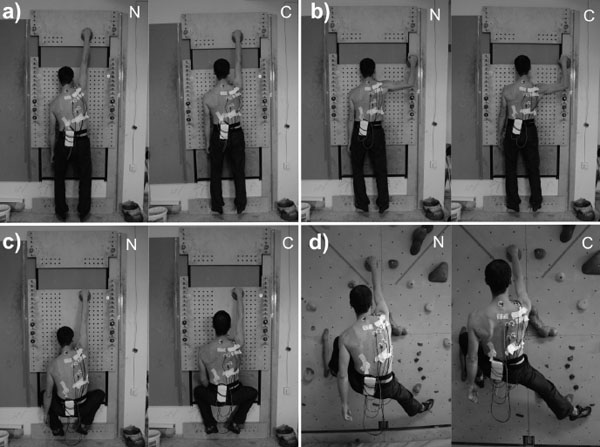
Surface EMG (TeleMyoMini 16, Neurodata, Germany) was used to assess muscle activity of the m. trapezius (inferior, middle, and superior part), m. serratus anterior, m. pectoralis major, and m. sternocleidomastoideus (Fig. 1). Participants completed all measurements in one day. After filling in an experience questionnaire, they performed a warm-up (five minutes aerobic exercises, five minutes traversing on the climbing wall, five minutes familiarisation with each climbing posture). The skin of the selected muscles was then cleaned with an alcohol to enhance surface EMG (SEMG) signal. Two electrodes were placed at the middle of each muscle belly, parallel to the muscle fibres. A common reference electrode was placed over the C7 spinous process. After preparation, each climber completed a maximal voluntary contraction (MVC) test for each of the selected muscles and measurement in each of the four climbing postures.
MVC Measurement
The MVC tests for the defined muscles were undertaken according to the protocol set out by Kendall et al. [10]. The contractions during the MVC lasted from 10-20 seconds and were repeated three times for each muscle with two minutes rest to avoid fatigue. The mean of the three highest amplitudes was considered as the reference SEMG amplitude for the MVC.
Climbing Postures
Four typical static postures were chosen for EMG measurement (Fig. 1). Participants wore climbing shoes to enable them to stand on the small footholds (1.5 cm deep). The same handhold was used for all four tested postures. The hold was sufficiently large as to allow non-climbers to hold each of the static postures for at least 30 sec. Each posture was set individually according to the length of body segments using a highly adjustable climbing wall. The SEMG activity was recorded twice for each of the two shoulder positions: naturally adopted position - climbers were asked to position themselves naturally in each of the described position; corrected position - instructions for the corrected position were given to keep the shoulder down with the medial edge of scapula parallel to the spine. Participants were required to hold each posture for 30 sec, with five min rest between each of the trials. The whole procedure (explanation, warm-up, MVC measurement, climbing positions measurement) for one participant lasted approximately 100-120 min. The testing of climbing positions was videoed and the recording was synchronised with the SEMG.
Description of postures:
- “Straight arms, straight legs”. Vertical wall. Standing position with right arm in shoulder flexion and elbow in full extension, legs extended in knees, feet spaced shoulder width (Fig. 1a).
- “Bent arm, straight legs”. Vertical wall. Bent knees and right arm in shoulder flexion and elbow in full extension, feet spaced shoulder width (Fig. 1b).
- “Straight arm, bent legs”. Vertical wall. Standing position with the shoulder in external rotation and abduction (90°), flexion in the elbow (90°), feet spaced shoulder width (Fig. 1c).
- “Overhang posture”. Overhanging wall (15° from the vertical). Left leg standing with a bent knee on foothold placed shoulder width distance left of the handhold and 90 cm down vertically. Right arm in shoulder flexion and elbow extension elbow, with the right leg flagging against the wall to support balance (Fig. 1d).
Data Analysis
SEMG data were recorded using MyoResearch XP software (Master Edition 1.08; Noraxon, USA) which enabled synchronisation with recorded video. The raw signal was rectified and smoothed by applying a root mean square with a window size of 100 ms. ECG filtering was used to correct the SEMG signal from the cardiac muscle activity. The SEMG muscle activity between the 10th sec and 20th sec was taken for further analysis. The mean SEMG amplitude was calculated and then normalised to MVC amplitude. Normalised SEMG were reported for all muscles in each position, separately for climbers and non-climbers. No statistical comparisons were made of climbers and non-climbers due to the small sample size. However, data for all participants (n = six) and for all postures (n = four) were compared for each muscle and differences were assessed by repeated measures ANOVA. Statistical significance was set to p ≤ 0.05. Partial omega squared (ωp2) was used to assess effect size of the differences. All analyses were calculated in Microsoft Excel and statistical software IBM SPPS 20.0 (Chicago, IL, USA).
RESULTS
Corrected shoulder position led to higher SEMG amplitude in m. trapezius –middle and lower parts, and m. sternocleidomastoideus than naturally chosen shoulder positions in all participants for the sum of all climbing postures Table 1. The highest SEMG amplitude was found with the m. trapezius – lower and middle part. Very low SEMG amplitude was identified for m. pectoralis major, m. sternocleidomastoideus, m. trapezius – superior part and m. serratus anterior. Muscles with SEMG activity lower than 10% MVC were not considered in further analyses – consequently, the sternocleidomastoid and upper trapezius were excluded from the comparison between climbers and non-climbers (Table 2).
| Muscle | Naturally chosen Shoulder position (% MVC) | Corrected shoulder position (% MVC) | p value | ωp2 |
|---|---|---|---|---|
| M.trapezius - superior part | 4.1 ± 2.7 | 4.5 ± 2.3 | 0.547 | -0.11 |
| M.trapezius - middle part | 18.4 ± 8.9 | 35.3 ± 11.8 | 0.015 | 0.67 |
| M.trapezius - inferior part | 30.1 ± 13.8 | 61.7 ± 15.4 | 0.004 | 0.79 |
| M. serratus anterior | 6.1 ± 3.8 | 9.1 ± 3.0 | 0.198 | 0.17 |
| M. sternocleidomastoideus | 3.8 ± 1 | 6.5 ± 1.0 | 0.014 | 0.68 |
| M. pectoralis major | 7.2 ± 4.2 | 10.8 ± 5.5 | 0.076 | 0.40 |
| SEMG activity (% MVC) | ||||
|---|---|---|---|---|
| Shoulder position in climbers | Shoulder position in non-climbers | |||
| “Straight arms, legs” | Naturally chosen | Corrected | Naturally chosen | Corrected |
| M.trapezius - middle part | 15.8 ± 10.3 | 22.8 ± 6.5 | 10.3 ± 4.3 | 24.9 ± 13.2 |
| M.trapezius - inferior part | 28.1 ± 24.7 | 30.1 ± 5.3 | 17.4 ± 4.9 | 51.5 ± 20.5 |
| M. serratus anterior | 4.4 ± 3 | 15.2 ± 4 | 13 ± 10.6 | 7.8 ± 2.4 |
| M. pectoralis major | 3.1 ± 2.1 | 11.7 ± 1.8 | 11.3 ± 1.8 | 9.2. ± 4.7 |
| “Bent arm, straight legs” | ||||
| M.trapezius - middle part | 33.9 ± 18 | 60.6 ± 14.6 | 16.1 ± 4.3 | 27.1 ± 7.9 |
| M.trapezius - inferior part | 49.4 ± 12.2 | 67.2 ± 26.5 | 48 ± 6.6 | 75.6 ± 15.4 |
| M. serratus anterior | 1.8 ± 0.8 | 10.6 ± 11.9 | 2.7 ± 0.7 | 7.3 ± 5.1 |
| M. pectoralis major | 1.4 ± 0.4 | 1.6 ± 0.4 | 2.7 ± 0.5 | 3.2 ± 0.2 |
| “Straight arm, bent legs” | ||||
| M.trapezius - middle part | 11.3 ± 3.7 | 35.5 ± 21.3 | 16.8 ± 1.1 | 28.2 ± 12.8 |
| M.trapezius - inferior part | 18.4 ± 8.3 | 52 ± 5.7 | 20.6 ± 3.4 | 69.4 ± 31.6 |
| M. serratus anterior | 3.1 ± 1.5 | 6.2 ± 4.5 | 5.0 ± 1.0 | 6.6 ± 0.4 |
| M. pectoralis major | 7.9 ± 3.6 | 18.7 ± 8.7 | 7.0 ± 4.7 | 15.3 ± 2.5 |
| “Overhang posture” | Naturally chosen | Corrected | Naturally chosen | Corrected |
| M.trapezius - middle part | 10.6 ± 2.9 | 40.9 ± 19.6 | 32.5 ± 3.4 | 42.7 ± 11.5 |
| M.trapezius - inferior part | 14.6 ± 2.9 | 65.9 ± 11.1 | 44 ± 15.7 | 81.5 ± 23.8 |
| M. serratus anterior | 4.2 ± 2.2 | 11.7 ± 7.9 | 4.3 ± 1.6 | 7.0 ± 1.2 |
| M. pectoralis major | 10.7 ± 2.7 | 12.5 ± 5.2 | 13.7 ± 4.2 | 14.3 ± 2.3 |
The middle trapezius activation was similar between climbers and non-climbers with the exception of the “Bent arm, straight legs” posture, where climbers demonstrated approximately two-fold higher SEMG mean amplitude than non-climbers. Generally, the “Bent arm, straight legs” posture for climbers and the “Overhang posture” for climbers and non-climbers with shoulder correction were identified to mostly stimulate activity of the middle trapezius, with SEMG amplitude exceeding 40% of MVC.
The lower trapezius was found to have systematically higher SEMG amplitude in non-climbers than in climbers for both the naturally chosen and corrected shoulder positions. High SEMG amplitude (> 60% MVC) was found in nearly all climbing postures with corrected shoulder placement except “straight arm, straight legs” posture. The m. serratus anterior demonstrated low SEMG activity during all static postures; generally, higher SEMG amplitude were found in climbers in positions with shoulder corrections, no SEMG amplitude exceeded 15% of MVC. The m. pectoralis major showed higher SEMG amplitude in shoulder corrected positions; there were no substantial differences between climbers and non-climbers, SEMG activity did not exceed 15% of MVC in any condition.
DISCUSSION
The main finding of the study was that there were differences in the activation of the scapula stabilizing muscles during static contraction in the two contrasting shoulder positions, uncorrected and corrected. The middle and lower trapezius demonstrated to have significantly higher SEMG activation for the corrected shoulder position in comparison to the naturally chosen shoulder position.
The greatest activation of lower trapezius was identified in the “bent arm, straight legs” and “overhanging” postures. These postures placed the support for the hand away from the line of gravitational forces, and required high horizontal forces to be developed in order to maintain equilibrium [11]. Climbing postures involving the external rotation of the shoulder at 90° abduction cause maximum depression of the scapula, isolating the upper and lower trapezius to a greater extent than any other exercise [12]. Interestingly, low activation of the upper trapezius was apparent in all climbing postures, and in both the natural and corrected condition. The low activation of the upper trapezius and high activation of middle and lower trapezius make these climbing postures interesting for rehabilitation programmes, where muscular imbalances between weak lower and middle trapezius and strong upper trapezius lead to scapulothoracic dysfunction [5].
Low serratus anterior SEMG activation was found for all postures with a non-significant increase in activation in corrected shoulder positions. The serratus anterior produces scapular upward rotation, posterior tipping, and external rotation, thus preserving the subacromial space [13]. Research has linked weakness in the serratus anterior muscle to shoulder pathology [14]. Therefore, exercises to strengthen the serratus anterior and develop coordination of its activity with the lower trapezius should be considered in climbing training programmes.
The pectoralis major is one of the strongest prime movers of the glenohumeral joint. Subjects with higher activation of pectoralis major and lower activation of serratus anterior during different push-up exercises have previously demonstrated scapular winding and, therefore, incorrect scapula positioning [15]. We hypothesised higher pectoralis major activation during naturally chosen shoulder positions, which was not confirmed. For all climbing postures, irrespective of shoulder position, very low activity of pectoralis major was recorded. However, the activation of pectoralis major may be different during dynamic climbing movements.
The sternocleidomastoid is superficial cervical flexor and takes over the role of deep cervical flexors during neck stabilizing tasks in patients with cervical disorders [16]. High activity of the sternocleidomastoid is often associated with a forward head posture and craniocervical pain [17]. Anecdotally, climbers often have poor posture, with the head held forward, rounded shoulders and lower cervical spine lordosis, although evidence-base for this dysfunctional posture in climbers is limited. Our results show very low activation of sternocleidomastoid during static climbing postures. Therefore, we cannot relate typical static climbing postures to a forward head posture. On the other hand, other climbing related activities such as belaying or spotting climber, due to the need to look upwards for extended periods of time, may induce high activity of sternocleidomastoid and induce impairment of the deep active stabilising system.
The climbers had similar recruitment patterns as the non-climbers, although non-climbers systematically showed greater lower trapezius SEMG activity. This might be due to lower upper body strength in the non-climbers, and, therefore, greater relative intensity when hanging on the same hold. However, this was not found for the middle trapezius.
The natural placement of the shoulder in elevation is in agreement with clinicians’ observations [1]. No subject maintained the gleno-humeral joint in a central position when asked to place themselves naturally in any of the static climbing postures; as this position was found to produce lower scapula stabilizing muscles activation, climbers should focus on centring the shoulder during actual climbing. On the other hand, using climbing postures while also centring the shoulder might be a suitable exercise after shoulder injuries, in rehabilitation or preventive programmes, as scapula stabilizing muscles are highly activated.
Several limitations should be acknowledged; the authors are aware that the small sample size limits the possibility of performing thorough statistical analyses. However, low variability in muscle activity between subjects was found, which supports the internal validity of the results. Results cannot be generalized to all climbing postures, as only four typical postures appearing in beginners and advanced climbers were assessed.
CONCLUSION
Climbers appear to naturally elevate their shoulder when adopting static climbing posture. This shoulder position induces lower activation of the scapula stabilizing muscles than when shoulder position correction is performed. Climbing with a corrected shoulder position may provide a suitable therapeutic exercise to develop lower and middle trapezius strength, as there was low activation of the upper trapezius.
LIST OF ABBREVIATIONS
| SEMG | = Surface electromyography |
| MVC | = Maximal voluntary contraction |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
No Animals/Humans were used for studies that are base of this research.
CONSENT FOR PUBLICATION
Not applicable.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
Declared none.

